TL;DR: A 2026 medRxiv preprint on schizophrenia reported that illness insight tracked with resting-state functional MRI (fMRI) flexibility, a measure of how dynamically brain regions reconfigure their connectivity, and that these brain-dynamics patterns aligned with dopamine D2 and serotonin 5-HT2A receptor maps after accounting for antipsychotic receptor occupancy.
Key Findings
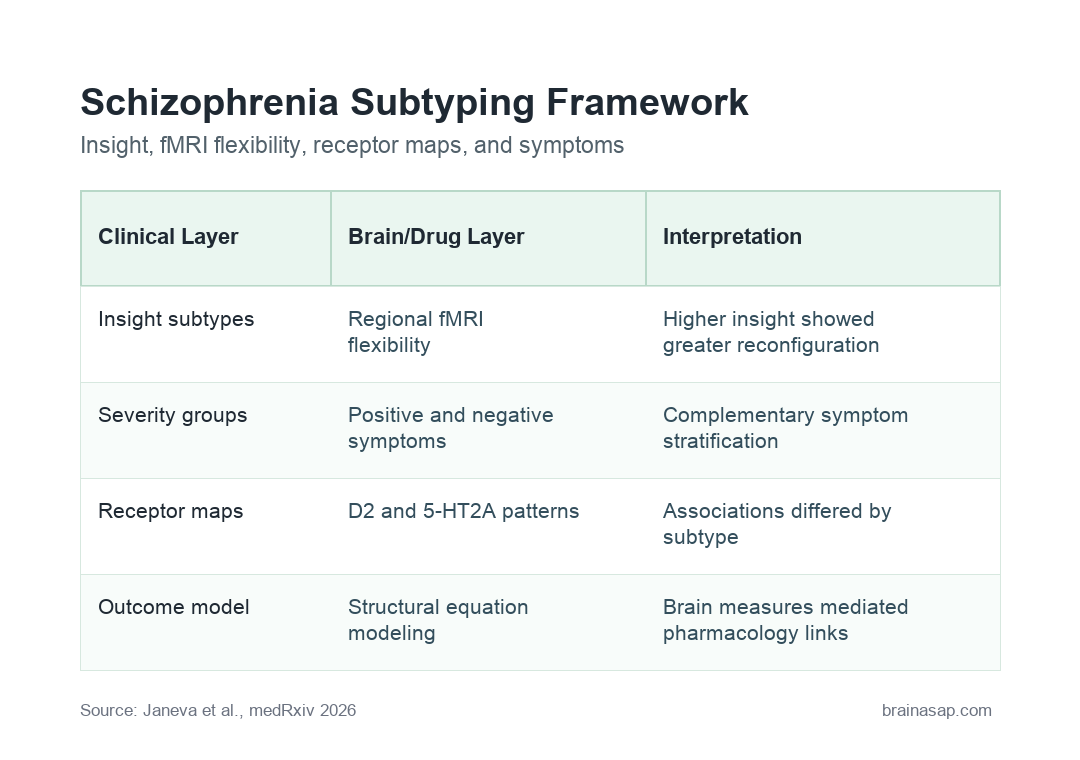
- Two insight subtypes: Clinical clustering identified two schizophrenia patient subtypes primarily differentiated by degree of illness insight.
- Three symptom-severity groups: A separate stratification used positive and negative psychopathology dimensions to define three severity groups.
- fMRI flexibility stood out: Higher-insight patients showed greater dynamic reconfiguration of regional functional connectivity, making flexibility the main neuroimaging feature separating insight subtypes.
- D2 and 5-HT2A maps aligned: Regional flexibility was spatially associated with cortical dopamine D2 and serotonin 5-HT2A receptor-density maps in subtype-specific patterns.
- Pharmacology linked to symptoms through brain dynamics: Structural equation modeling suggested that neuroimaging measures mediated the influence of receptor pharmacology on clinical outcomes.
Source: medRxiv (2026) | Janeva et al.
Schizophrenia insight means how well a person recognizes their illness, symptoms, and need for treatment. It is clinically important because insight can affect medication adherence, risk assessment, therapeutic alliance, and how clinicians interpret symptom reports.
This preprint asked whether insight and symptom severity could be tied to measurable brain-dynamics and pharmacology patterns rather than treated as one broad schizophrenia category.
Schizophrenia Subtypes Were Split by Insight and Symptom Severity
Schizophrenia is not one uniform biological state. Patients can share the same diagnosis while differing in hallucinations, delusions, negative symptoms, cognition, social functioning, medication response, and awareness of illness.
Researchers used multidimensional clinical features to look for patient groupings. The clustering analysis found two clinically meaningful subtypes, with illness insight as the main separator.
Researchers also used a second framework based on symptom severity. Positive symptoms include experiences such as hallucinations or delusions, while negative symptoms include reduced motivation, social withdrawal, or blunted emotional expression.
- Insight grouping: Two patient subtypes were mainly separated by how much illness insight they showed.
- Severity grouping: Three additional groups were defined from positive and negative psychopathology dimensions.
- Complementary view: Insight and symptom severity gave different but related ways to parse schizophrenia heterogeneity.
Resting-State fMRI Flexibility Distinguished Higher-Insight Patients
The main brain-imaging result involved resting-state fMRI, which measures brain activity while a person is not performing a specific task. Researchers used it to study regional functional connectivity, meaning how strongly brain areas fluctuate together over time.
The key measure was regional flexibility. Here, flexibility describes how much a brain region changes its network relationships across time instead of staying locked into one connectivity pattern.
Higher-insight patients showed greater dynamic reconfiguration of regional functional connectivity. The preprint describes this as the primary neuroimaging feature that differentiated the insight-based subtypes.
More flexibility is not automatically good in every brain region or every patient. In this dataset, insight was tied to a more dynamic pattern of regional connectivity.
Dopamine D2 and Serotonin 5-HT2A Maps Added Pharmacology Context
The pharmacology layer focused on receptor systems that are central to schizophrenia treatment. Dopamine D2 receptors are a major target of many antipsychotic drugs, while serotonin 5-HT2A receptors are also relevant to several atypical antipsychotics and psychosis biology.
Researchers compared regional flexibility patterns with cortical receptor-density maps. These maps estimate where receptor types are more or less densely represented across the cortex.
The associations were subtype-specific. In other words, the relationship between brain-network flexibility and receptor maps differed depending on the clinical subgroup being analyzed.
The analysis also accounted for estimated antipsychotic receptor occupancy. Receptor occupancy refers to the estimated proportion of receptors occupied by a medication at a given exposure, which matters when comparing patients taking different antipsychotic regimens.
- D2 context: Dopamine D2 receptor occupancy is closely tied to antipsychotic effect and side-effect risk.
- 5-HT2A context: Serotonin 5-HT2A signaling is relevant to atypical antipsychotic pharmacology and cortical function.
- Subtype context: Receptor-brain associations were stronger and more spatially widespread in specific patient subtypes.
Structural Equation Modeling Linked Receptors, Brain Dynamics, and Symptoms
The preprint did not stop at separate clinical, imaging, and pharmacology findings. Researchers used structural equation modeling, a statistical method for testing relationships among linked variables, to ask whether neuroimaging measures sat between receptor pharmacology and clinical outcomes.
In the reported model, neuroimaging measures mediated receptor pharmacology’s influence on clinical outcomes.
Mediation language needs caution. It does not prove that changing receptor occupancy will necessarily change fMRI flexibility and then improve symptoms in a simple chain.
It means the statistical model fit a pathway in which brain-dynamics measures helped explain the pharmacology-clinical relationship.
That is still a meaningful precision-psychiatry result. It suggests schizophrenia subtyping may be stronger when clinical features, imaging dynamics, and medication pharmacology are analyzed together.
Why Insight-Based Schizophrenia Subtyping Could Matter
Insight is often treated as a clinical observation. A brain-dynamics link would make it more biologically interpretable, especially if future studies can reproduce the flexibility pattern in independent cohorts.
For treatment research, this approach could help identify subgroups whose symptoms relate more strongly to particular receptor systems. That would fit the clinical reality that antipsychotic response and adverse effects vary widely across patients.
It also keeps medication exposure visible. In schizophrenia imaging studies, medication can be treated as a nuisance variable, but antipsychotics act directly on the receptor systems being studied.
Estimating receptor occupancy makes the drug signal part of the biological model instead of leaving it as a background adjustment.
This does not solve the full heterogeneity problem. It narrows the research target: which clinical subgroup, under which medication-exposure pattern, shows which brain-dynamics profile?
- Clinical targeting: Insight-defined subtypes may help researchers avoid averaging together biologically different patients.
- Medication interpretation: Receptor-occupancy estimates make medication exposure part of the model instead of background noise.
- Biomarker development: fMRI flexibility could become a candidate marker for subgrouping, though it is not ready for routine care.
The Main Limit Is Preprint-Level Evidence
This is not a clinical test for schizophrenia subtypes. The source is a preprint, and the available capture gives abstract-level methods and results rather than enough detail to audit sample size, scanner protocol, medication-dose assumptions, or model robustness.
Resting-state fMRI can also be sensitive to motion, preprocessing choices, medication state, illness duration, and cohort composition. Those factors matter when a finding depends on dynamic connectivity.
Medication timing is especially important here because the same analysis links brain dynamics to receptor pharmacology. A future replication would need to show that the flexibility pattern is not just a byproduct of who was taking which drug at which estimated receptor exposure.
The study’s practical value will depend on replication. Future work should test whether the same insight-linked flexibility pattern appears in independent samples and whether it predicts treatment response better than clinical measures alone.
- Design caveat: The analysis is observational and model-based, so causal treatment claims are not warranted.
- Measurement caveat: Dynamic fMRI metrics need careful validation before they can guide individual care.
- Source caveat: Peer review and fuller methods inspection are still needed.
The core contribution is a framework: schizophrenia subtypes may become more informative when clinical insight, symptom dimensions, brain-network flexibility, and receptor pharmacology are modeled in the same system.
Citation: DOI: 10.64898/2026.04.30.26352132; Janeva et al.; Insight and symptoms severity in schizophrenia explained by the flexibility of brain dynamics and pharmacological treatment; medRxiv; 2026;2026.04.30.26352132.
Study Design: Preprint observational modeling study integrating schizophrenia clinical subtyping, resting-state fMRI dynamics, receptor-density maps, antipsychotic receptor occupancy estimates, and structural equation modeling.
Sample/Model: Schizophrenia patient data from Aix-Marseille University-affiliated clinical and neuroimaging work; exact sample size was not available in the captured source text.
Key Statistic: Higher-insight patients showed greater dynamic reconfiguration of regional functional connectivity, and flexibility patterns aligned with D2 and 5-HT2A receptor maps in subtype-specific ways.
Caveat: Preprint and abstract-level public information; independent replication and full methods review are needed before clinical use.