TL;DR: A 2026 systematic review in Preventive Medicine Reports found limited but suggestive randomized-trial evidence that smoking-cessation medications can help Indigenous adults quit, especially when paired with supportive or culturally tailored care.
Key Findings
- 5 RCTs: The review found only 5 randomized controlled trials, totaling 1,633 participants, in American Indian, Alaska Native, and Maori adult populations.
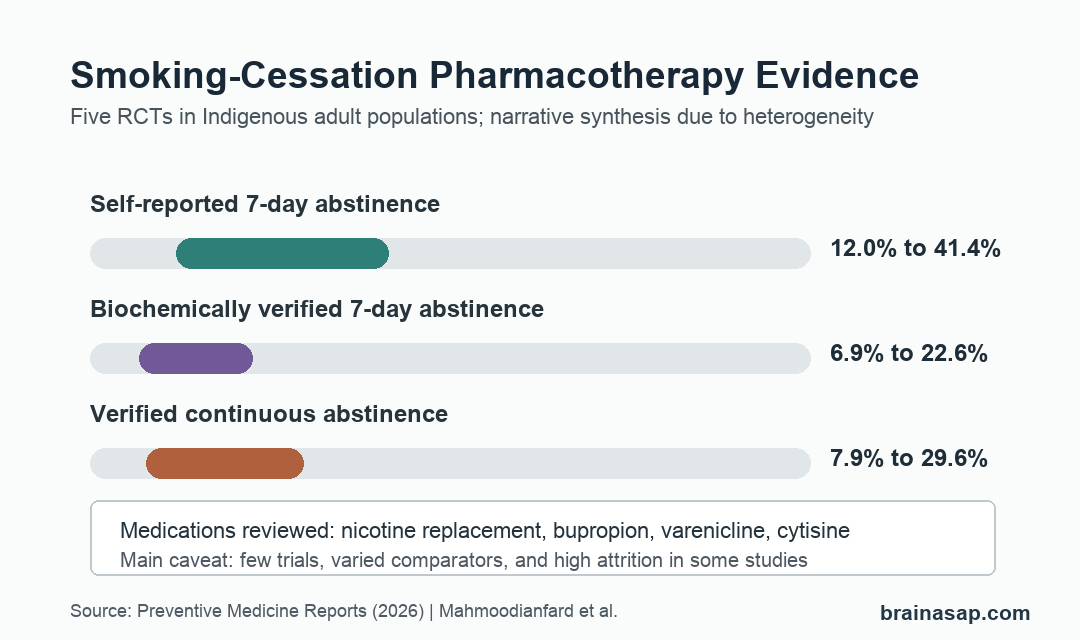
- 4 medication types: Trials included nicotine replacement therapy, bupropion, varenicline, and cytisine, alone or with behavioral or culturally tailored support.
- 12.0% to 41.4% self-reported quitting: Six-month self-reported 7-day point-prevalence abstinence varied widely across studies.
- 6.9% to 22.6% verified quitting: Biochemically verified 7-day abstinence at 6 months was lower than self-report, showing why verification changes interpretation.
- High attrition limited certainty: Adherence was generally high and adverse events were mild, but heterogeneity and high dropout constrained interpretation.
Source: Preventive Medicine Reports (2026) | Mahmoodianfard et al.
Commercial tobacco use carries a high health burden in many Indigenous communities, yet medication trials in these populations are relatively scarce. The review focuses on that evidence gap rather than treating general-population cessation results as automatically transferable.
Across multiple databases, the search found only 5 eligible randomized trials, leaving a cautious signal rather than a settled clinical playbook.
Only 5 Randomized Trials Met the Review Criteria
The review searched MEDLINE, Embase, CENTRAL, APA PsycINFO, Informit Indigenous Collection, Bibliography of Indigenous Peoples in North America, and Global Health. Searches ran in June to September 2024, with most sources updated on May 28, 2025.
That large search yielded 9,940 references. After duplicate removal and screening, researchers assessed 277 full-text articles and excluded 272, leaving 5 randomized controlled trials.
- Populations: 3 trials enrolled American Indian or Alaska Native adults, and 2 were conducted in Maori populations in New Zealand.
- Total sample: The trials included 1,633 participants, with individual study sizes ranging from 103 to 679.
- Participant profile: Participants were adult daily smokers who were motivated to quit, and most study samples were majority women.
- Follow-up: Study follow-up ranged from 3 to 18 months, making direct comparison difficult.
This screening result is itself a finding. The paper shows that medication-based smoking cessation for Indigenous adults has been tested in randomized trials, but not often enough to support broad certainty across communities, medications, and delivery models.
Nicotine Replacement, Bupropion, Varenicline, and Cytisine Were Studied
The medication set was clinically familiar: nicotine replacement therapy, bupropion, varenicline, and cytisine. The trials differed in whether medication was the main comparison or was given alongside counseling or other support.
Some trials tested culturally tailored behavioral programs layered onto medication. Others compared medication choices more directly, such as cytisine versus varenicline with brief support.
- Medication plus tailoring: One American Indian/Alaska Native trial compared All Nations Breath of Life counseling plus pharmacotherapy with non-tailored current best practices plus pharmacotherapy.
- Varenicline support: Another trial compared culturally tailored treatment with standard treatment while both groups used varenicline.
- Bupropion trial: A Maori study compared bupropion plus culturally adapted counseling with placebo plus counseling.
- Cytisine comparison: A pragmatic trial compared 12 weeks of cytisine with 12 weeks of varenicline, both with brief support.
Because the support structures varied so much, the review synthesized results narratively instead of pooling them into a single meta-analysis. A single averaged effect would have hidden major design differences.
Verified Abstinence Was Lower Than Self-Reported Quitting
At 6 months, self-reported 7-day point-prevalence abstinence ranged from 12.0% to 41.4%. Biochemically verified 7-day abstinence ranged from 6.9% to 22.6%.
That gap is important. Self-report can be useful, but carbon monoxide or cotinine verification gives a stricter measure of quitting and often lowers the apparent success rate.
- Culturally tailored counseling trial: In 1 American Indian/Alaska Native study, self-reported 6-month abstinence was 20.1% versus 12.0%, but cotinine-verified abstinence was 10.8% versus 6.9%.
- Varenicline trial: Another study reported carbon monoxide-verified six-month 7-day abstinence of 14.0% versus 22.6%, with no significant difference between groups.
- Cytisine versus varenicline: Six-month self-reported 7-day abstinence was 41.4% versus 32.9%, while verified continuous abstinence was 12.1% versus 7.9%.
The review also reported biochemically verified continuous abstinence from 7.9% to 29.6% at 6 months. Continuous abstinence is stricter because it asks whether abstinence continued, not only whether the person was abstinent during a short recent window.
Cytisine and Bupropion Had Notable Trial Signals
The cytisine trial was the largest included study, with 679 participants. Self-reported outcomes generally favored cytisine over varenicline, including 6-month 7-day abstinence of 41.4% versus 32.9% with a relative risk of 1.26.
The bupropion trial also showed a strong early signal. In that Maori study, carbon monoxide-verified continuous abstinence at 3 months was 44.3% with bupropion versus 17.4% with placebo, and 6-month rates were 29.6% versus 10.9%.
- Cytisine tolerability: The cytisine arm had 44% fewer adverse events than varenicline, with an incidence rate ratio of 0.56.
- Bupropion side effects: Insomnia was more common with bupropion, reported as 26% versus 9%.
- Safety summary: Across trials, adverse events were generally mild and consistent with known cessation-medication effects.
These medication signals are promising, but they should not be overread. The review was not a large pooled efficacy analysis, and each trial sat inside a specific cultural, clinical, and support context.
Community-Led Trials Are the Main Evidence Gap
The review’s most practical conclusion is not that 1 medication is clearly best. Medication access, cultural fit, behavioral support, and retention all need to be studied together.
Attrition was a major limitation. One included trial had more than 90% attrition, and the broader evidence base was too heterogeneous for a single pooled estimate.
- Few trials: 5 RCTs cannot represent the full range of Indigenous communities, health systems, and smoking-cessation needs.
- Different comparators: Some studies compared support models while both arms received medication, so medication-specific effects were hard to isolate.
- Outcome inconsistency: Trials used different definitions, time points, and verification methods.
- Implementation context: Cost, remote access, trust, side effects, and alignment with community-based healing can affect whether medication is used and continued.
The evidence supports offering proven cessation medications with care that fits the community context. It also supports a research priority: larger community-led randomized trials that test medication, support, verification, and retention as connected parts of the intervention.
Citation: DOI: 10.1016/j.pmedr.2026.103460. Mahmoodianfard et al. Pharmacotherapies for smoking cessation among Indigenous Peoples: A systematic review of randomized controlled trials. Preventive Medicine Reports. 2026;65:103460.
Study Design: Systematic review of randomized controlled trials evaluating smoking-cessation pharmacotherapies among Indigenous adults.
Sample Size: 5 RCTs with 1,633 total participants from American Indian, Alaska Native, and Maori populations.
Key Statistic: Six-month self-reported 7-day abstinence ranged from 12.0% to 41.4%, while biochemically verified 7-day abstinence ranged from 6.9% to 22.6%.
Caveat: The evidence base was small and heterogeneous, with high attrition in some studies and varied medication, counseling, and verification designs.