TL;DR: A 2026 medRxiv preprint found that stroke thrombectomy operators often had a preferred device technique, but that preference did not reliably match the technique with the highest first-pass reperfusion rate.
Key Findings
- Stroke thrombectomy cohort: The single-center analysis included 1,405 acute ischemic stroke patients treated with mechanical thrombectomy from 2019 through 2024.
- 75% had a preference: Most operators used one thrombectomy technique for more than half of their cases in a study period.
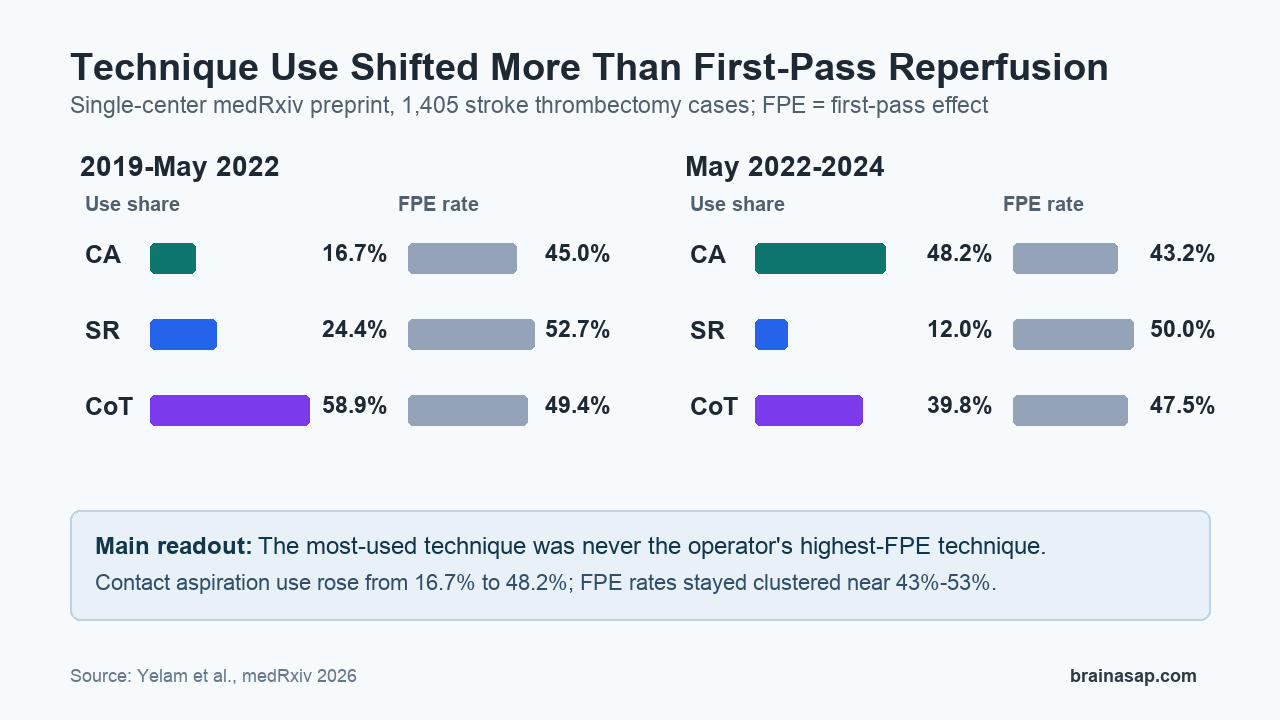
- Preference did not predict best FPE: For every operator, the most-used technique was never the technique with the highest first-pass effect rate.
- Technique mix shifted: Contact aspiration increased from 16.7% of cases in 2019-May 2022 to 48.2% in May 2022-2024.
- Contact aspiration learning curve: Among newer operators, increasing case volume was linked to better first-pass effect only for contact aspiration.
Source: medRxiv (2026) | Yelam et al.
Mechanical thrombectomy is a catheter-based procedure used to remove large clots during acute ischemic stroke. For selected patients, reopening the blocked artery quickly can limit brain injury and improve the chance of recovery.
This preprint focused on a narrower technical question: when neurointerventionists prefer one thrombectomy approach, does that preference line up with better first-pass reperfusion?
First-pass effect (FPE) means achieving strong reperfusion after the first device pass. It matters because fewer passes can mean shorter procedures, less vessel manipulation, and potentially better clinical outcomes.
Three Thrombectomy Techniques Were Compared
The researchers analyzed prospective thrombectomy data from a comprehensive stroke center. Eligible patients had large vessel occlusion strokes treated with one of three approaches: contact aspiration, stent retriever, or a combined technique.
Contact aspiration uses suction through a catheter to remove the clot. Stent retriever treatment deploys a device through the clot and pulls it back. Combined technique uses aspiration plus stent retriever.
- Study period: 2019 through 2024, split into 2019-May 2022 and May 2022-2024.
- Included cases: 1,405 thrombectomy patients out of 1,612 treated during the period.
- Main endpoint: First-pass effect rate by operator and technique.
A preferred technique was defined as a technique used in more than half of an operator’s thrombectomy cases during a period. That definition makes the study practical: it asks whether real procedural habits tracked with measured performance.
Operators Often Had a Preferred Technique
Technique use changed substantially over time. In the first period, the combined technique was most common, used in 58.9% of cases. Stent retriever accounted for 24.4%, and contact aspiration accounted for 16.7%.
By the second period, contact aspiration had become the most-used approach at 48.2%. Combined technique fell to 39.8%, and stent retriever declined to 12.0%.
Most operators had a clear procedural preference. The paper reported that 75.0% of operators used one technique for more than half of their cases in a period.
That preference pattern is clinically plausible. Operators may favor a device strategy because of training, local workflow, perceived speed, vessel anatomy, clot appearance, device availability, or prior cases that shaped their confidence.
Preferred Technique Was Not the Highest-FPE Technique
No technique dominated across operators; instead, use and performance often diverged.
For each individual operator, the technique with the highest FPE rate was never the most commonly used technique. Because case selection, anatomy, and other procedural factors were not fully controlled, this mismatch cannot identify the best technique for every case; it does show that habitual use alone was not a reliable performance marker.
Across techniques, increased use was not clearly associated with higher FPE. The odds ratio per percentage-point increase in use was 1.04 for contact aspiration, 1.01 for combined technique, and 1.00 for stent retriever, with confidence intervals crossing no clear effect.
Previous cumulative success with a technique also did not significantly improve prediction of the next case’s FPE. The model comparison was not significant, with chi-square = 6.46, df = 3, and p = 0.09.
Contact Aspiration Showed a Learning Curve
The study did find one technique-specific learning signal among newer operators. Overall, increasing case volume was associated with higher FPE, with beta = 0.021 and p = 0.006.
When the researchers separated techniques, only contact aspiration showed a significant learning curve. Contact aspiration had a positive slope of 0.004 with p < 0.01.
- Contact aspiration: FPE improved as newer operators accumulated cases.
- Stent retriever: No significant volume-FPE association was detected, though the new-operator sample was small.
- Combined technique: No significant association between case volume and FPE was detected.
This was a learning-curve signal rather than a head-to-head inferiority result. Performance with contact aspiration may depend on case accumulation and device-specific optimization, especially as catheter technology changes.
Bleeding Rates Did Not Clearly Differ by Technique
Safety analyses focused on parenchymal hematoma, a serious bleeding complication after ischemic stroke treatment. For individual operators, parenchymal hematoma rates did not significantly differ across thrombectomy techniques in pairwise comparisons.
The main exception was a lower parenchymal hematoma rate for stent retriever compared with contact aspiration for one operator, but that stent retriever subgroup had only 3 cases. The paper treated that as too small for a broad safety conclusion.
In the full cohort, the supplemental baseline table reported 660 FPE events, equal to 47.0% of cases. Modified first-pass effect occurred in 882 cases, or 62.8%.
- Final TICI 2c-3: 1,063 cases, or 75.6%, reached near-complete or complete final reperfusion.
- PH1: 73 cases, or 5.2%, had parenchymal hematoma type 1.
- PH2: 52 cases, or 3.7%, had parenchymal hematoma type 2.
The Preprint Does Not Set a Bedside Rule
The results should not be read as a simple recommendation to abandon preferred techniques. Thrombectomy choices can depend on vessel anatomy, clot composition, access route, device inventory, prior imaging, and the operator’s judgment during the case.
Teams should therefore compare their favored technique with local, case-adjusted outcomes instead of assuming that the most-used approach is also the best-performing one.
The study also has important limits. It came from a single high-volume center, had no core-lab imaging adjudication, and could not fully account for clot biology, stroke etiology, evolving aspiration-catheter technology, or the detailed procedural choices behind each technique label.
Because the analysis is a preprint, it has not been certified by peer review and should not guide clinical practice on its own. Its appropriate role is to prompt quality review: track operator-level technique use, first-pass reperfusion, safety events, and case mix before assuming that preference equals performance.
Citation: DOI: 10.64898/2026.07.01.26357084. Yelam et al. Impact of Operator Technique Preference on Thrombectomy Reperfusion Outcomes. medRxiv. 2026.
Study Design: Retrospective analysis of prospective data from a single comprehensive stroke center.
Sample Size: 1,405 acute ischemic stroke patients treated with mechanical thrombectomy.
Key Statistic: The most-used technique was never the highest-FPE technique for individual operators.
Caveat: This is a non-peer-reviewed preprint from one center, and technique selection may reflect case anatomy, clot features, and operator judgment.