TL;DR: A 2026 systematic review in Translational Psychiatry found that depression brain-stimulation studies repeatedly linked treatment response to subcallosal cingulate connectivity, but inconsistent methods still limit its use as a treatment-selection biomarker.
Key Findings
- 28 studies met criteria: The review included resting-state functional MRI (fMRI), a scan that tracks blood-flow changes as a proxy for brain activity, studies of subcallosal cingulate connectivity after brain stimulation for depression.
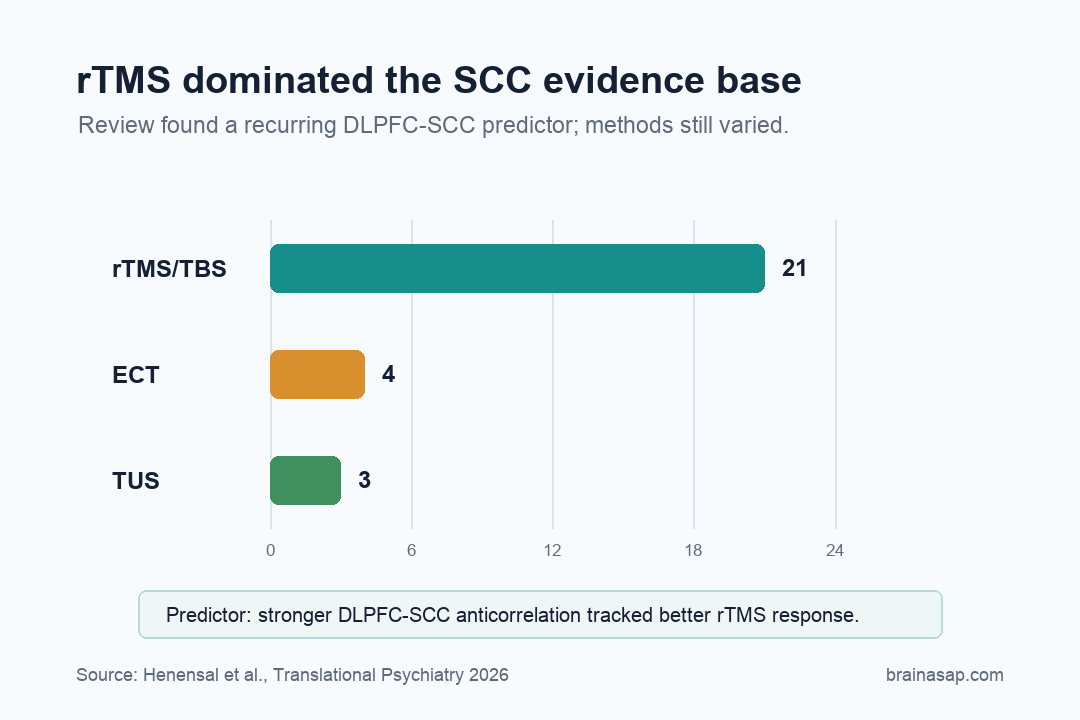
- rTMS dominated the evidence: Repetitive transcranial magnetic stimulation (rTMS), a noninvasive treatment that uses magnetic pulses to stimulate cortex, or theta-burst stimulation appeared in 21 studies; ECT appeared in 4 and focused ultrasound in 3.
- DLPFC-SCC coupling stood out: Stronger baseline anticorrelation between the dorsolateral prefrontal cortex and subcallosal cingulate often predicted better rTMS response.
- ECT findings were less consistent: ECT studies reported heterogeneous changes involving temporal, ventromedial prefrontal, amygdala, and supramarginal regions.
- Focused ultrasound is early but intriguing: Three TUS studies reported changes in SCC connectivity, including links with the DLPFC, medial prefrontal cortex, hippocampus, and cerebellum.
- Standardization is the bottleneck: Different SCC definitions, stimulation protocols, and analysis methods make it difficult to turn the connectivity finding into a clinical rule.
Source: Translational Psychiatry (2026) | Henensal et al.
Treatment-resistant depression creates a strange targeting problem. Clinicians stimulate one part of the brain, symptoms improve in some patients, and the decisive marker may come from subcallosal cingulate connectivity in a deeper region that was never directly touched.
The Subcallosal Cingulate Is the Deep Mood Hub
The subcallosal cingulate is a small deep-brain region tucked below the corpus callosum. It has become one of depression research’s recurring suspects because it sits at the crossroads of mood, self-referential thought, autonomic state, and limbic regulation.
In major depressive episodes, the region often behaves abnormally. That has made it a candidate target for deep brain stimulation and focused ultrasound, and a possible downstream node for treatments aimed at the dorsolateral prefrontal cortex.
The review asked a practical question: when brain stimulation helps depression, what happens to subcallosal cingulate functional connectivity?
Functional connectivity means that two brain regions fluctuate together over time, as measured with resting-state fMRI.
Modern depression treatment is increasingly network-based. A coil, electrode, or ultrasound focus may be placed in one location, but the therapeutic effect can depend on how that location is wired to deeper mood circuits.
The SCC is one of the places where those wires keep reappearing.
Most of the Evidence Comes From rTMS
Researchers screened the literature through December 15, 2025 and included 28 studies. The evidence base was heavily weighted toward rTMS and theta-burst stimulation, with 21 studies in that category.
ECT contributed four studies, and transcranial ultrasound contributed three.
No tDCS or DBS studies met the review’s criteria for pre/post resting-state fMRI connectivity involving the subcallosal cingulate. The imaging evidence needed for this specific question was missing, even though those methods can still be relevant to depression treatment.
- 21 studies: rTMS or theta-burst stimulation, the dominant evidence base in the review.
- 4 studies: electroconvulsive therapy, with more heterogeneous SCC-connectivity findings.
- 3 studies: focused ultrasound, an early but deeper-reaching stimulation approach.
Across rTMS studies, SCC connectivity changes touched several network partners:
- Frontal regions: dorsolateral prefrontal and orbitofrontal areas tied to control and mood regulation.
- Default-mode regions: precuneus and related self-referential networks.
- Limbic regions: hippocampal and deeper mood-circuit partners.
The findings were not perfectly uniform, but one relationship stood out: the link between the DLPFC and SCC.
The review did not run a meta-analysis because too few studies used comparable methods within each stimulation category. That choice kept the review from forcing a single pooled effect out of mismatched designs.
Instead, the researchers mapped where the evidence repeatedly points.
The Predictor Was an Opposing Pattern
Several rTMS studies found that patients did better when the stimulation target in the dorsolateral prefrontal cortex was more strongly anticorrelated with the subcallosal cingulate before treatment.
Those regions were already fluctuating in opposite directions.
rTMS is delivered at the surface. If a prefrontal target is naturally opposed to the deep depression hub, stimulating it may be more likely to push the network in the desired direction.
Put less technically, the best surface target is the one with the strongest line of influence into the deeper circuit. The treatment is delivered to cortex, but the depression-relevant change may require shifting activity in the SCC and its limbic partners.
The idea has already influenced personalized targeting strategies. Some groups try to choose a DLPFC stimulation site based on its individual connectivity with the subcallosal cingulate.
The review supports that logic, while also warning that it is not yet a settled clinical rule.
There is a real tension here. Personalized targeting sounds better than one-size-fits-all stimulation, but it depends on stable imaging measures and reproducible analysis.
If two labs define the SCC differently, they may be personalizing different circuits.
The same caution applies to response prediction. A connectivity pattern that looks powerful in a carefully selected research sample may weaken in a broader clinic population.
The marker has to travel across several real-world complications:
- Comorbid anxiety: overlapping symptoms and circuitry can blur depression-specific prediction.
- Medication differences: drug histories may alter resting-state connectivity before stimulation begins.
- Depression chronicity: long illness duration may shift network biology and treatment response.
- Mixed stimulation histories: prior rTMS, ECT, or other interventions can change the baseline network being measured.
ECT and Ultrasound Added Less Consistent SCC Evidence
ECT remains one of the most effective treatments for severe depression, but its subcallosal cingulate connectivity results were heterogeneous in this review. Studies reported changes involving the temporal pole, parahippocampal regions, ventromedial prefrontal cortex, amygdala, and supramarginal gyrus.
Focused ultrasound is newer and smaller as an evidence base. One study targeting the SCC reported increased connectivity with the DLPFC.
Other ultrasound studies targeting the DLPFC found altered connectivity among SCC subregions, medial prefrontal cortex, and cerebellum.
Ultrasound is intriguing but early. It can reach deeper targets than standard magnetic stimulation, but the field still needs larger studies with consistent imaging definitions and clinical endpoints.
Different SCC Definitions Keep Blurring the Finding
The review’s main warning is methodological. Studies defined the subcallosal cingulate differently, used different seed regions, applied different stimulation protocols, and analyzed connectivity in different ways.
- SCC definition: different anatomical boundaries can point to different tissue.
- Seed choice: connectivity results depend on the starting region used in the analysis.
- Protocol variation: stimulation dose, site, and timing differed across studies.
- Analysis pipeline: preprocessing and statistical choices can change the reported network pattern.
That kind of variation can make a real biological relationship look unstable. It can also make a weak finding look stronger than it is.
Before SCC connectivity can guide everyday treatment selection, the field needs shared definitions and reproducible pipelines.
The SCC is also technically difficult to measure. It is small, deep, and more vulnerable to lower fMRI image quality than many cortical regions.
The promise of SCC connectivity therefore comes with a higher quality-control burden.
Here, the review is strongest. It does not oversell connectivity as a ready-made clinical test.
It argues that the same hub keeps showing up, then explains why the current evidence is not yet clean enough to dictate care.
A Pre-Treatment DLPFC-SCC Scan Is Not Clinic-Ready Yet
The review does not show that a brain scan can now pick the best stimulation treatment for depression. It suggests the field is closing in on a plausible network marker, especially for prefrontal rTMS.
The subcallosal cingulate should be treated as a deep network hub, not a single button. If future studies can standardize how that hub is measured, depression stimulation can become less trial-and-error and more network-guided.
For patients, that would be a meaningful shift. Treatment-resistant depression often forces people through long sequences of medication changes, stimulation protocols, and waiting periods.
A reliable network marker would not eliminate uncertainty, but it could make the first target smarter.
The most realistic near-term goal is not a universal depression scan. It is a better rule for selecting and positioning stimulation in people already being considered for neuromodulation.
That is a narrower claim, but it is also the one the evidence can actually support.
Citation: DOI: 10.1038/s41398-026-03999-3. Henensal et al. Subcallosal cingulate functional connectivity in depression: a systematic review of brain stimulation-induced changes and pretreatment connectivity predictors. Translational Psychiatry. 2026.
Study Design: Systematic review of resting-state fMRI connectivity studies after brain stimulation for depression.
Sample Size: 28 studies met criteria: 21 examined rTMS or theta-burst stimulation, 4 examined ECT, and 3 examined focused ultrasound.
Key Statistic: Stronger baseline anticorrelation between DLPFC stimulation targets and the subcallosal cingulate often predicted better rTMS response.
Caveat: The review did not run a meta-analysis because stimulation protocols, SCC definitions, and connectivity methods were too heterogeneous.