TL;DR: A 2025 systematic review in Translational Psychiatry found that substance use disorder was associated with recurring resting-state functional MRI (rs-fMRI), a scan of spontaneous brain-network communication, abnormalities in reward and self-control circuits across 53 studies.
Key Findings
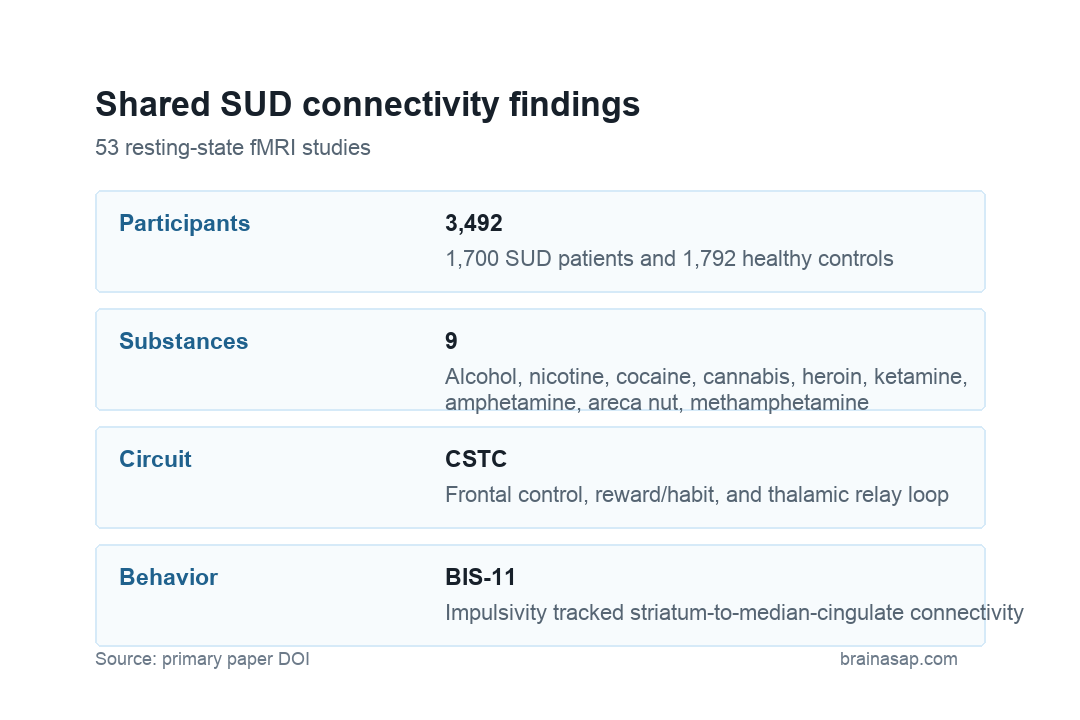
- 53-study meta-analysis: Researchers pooled whole-brain rs-fMRI studies covering 1,700 people with substance use disorder and 1,792 healthy controls.
- Nine substances: Included studies covered alcohol, nicotine, cocaine, cannabis, heroin, ketamine, amphetamine, areca nut, and methamphetamine.
- Reward circuit focus: The analysis tested connectivity from the anterior cingulate cortex, prefrontal cortex, striatum, thalamus, and amygdala.
- CSTC disruption: The cortical-striatal-thalamic-cortical (CSTC) circuit, a loop linking frontal control regions, reward circuitry, and thalamic relay functions, showed recurring dysfunction.
- Impulsivity link: Weaker striatum-to-median-cingulate connectivity was negatively correlated with Barratt Impulsiveness Scale-11 (BIS-11) scores, a questionnaire measure of impulsive behavior.
Source: Translational Psychiatry (2025) | Zhang et al.
Substance use disorder is clinically diverse, but many forms share loss of control, compulsive seeking, craving, and impaired decision-making. Those symptoms point toward brain systems that process reward, habit learning, emotional salience, and executive control.
Resting-state functional connectivity measures how brain regions fluctuate together while a person is awake and not performing a task. The method cannot prove cause, but it can identify network differences that recur across studies and substances.
Substance Use Disorder Shared Reward-Circuit Connectivity Changes
The meta-analysis focused on five seed regions that are central to addiction neuroscience: the anterior cingulate cortex, prefrontal cortex, striatum, thalamus, and amygdala. Researchers used seed-based d mapping to look for common whole-brain connectivity changes from those regions.
The pooled sample was large for neuroimaging: 1,700 substance use disorder patients and 1,792 controls. Individual studies still differed in substance type, abstinence stage, demographic balance, and psychiatric exclusions, so the pooled maps should be read as recurring network features rather than a single diagnostic signature.
- Frontal control: Prefrontal and inferior frontal connections are relevant to planning, inhibition, and decision-making.
- Reward and habit: Striatal connections are relevant to motivation, reward learning, and compulsive use.
- Emotion and memory: Amygdala and parahippocampal findings point toward emotional salience and drug-cue memory.
CSTC Circuit Dysfunction Linked Frontal Control With Reward Processing
The cortical-striatal-thalamic-cortical circuit appeared repeatedly in the analysis. That loop connects frontal cortex, striatum, thalamus, and back to cortex, giving it a plausible role in the tension between immediate reward and longer-term control.
Several directions were reported. The prefrontal cortex showed hyperconnectivity with the superior frontal gyrus and striatum, along with hypoconnectivity with the inferior frontal gyrus. The striatum showed hyperconnectivity with the superior frontal gyrus and hypoconnectivity with the median cingulate gyrus.
Impulsivity Scores Tracked Striatum-to-Cingulate Connectivity
The behavioral association was narrow but clinically relevant. Reduced resting-state connectivity between the striatum and median cingulate gyrus was negatively correlated with BIS-11 impulsivity scores. In practical terms, weaker connectivity in that pathway went with higher impulsivity scores.
The scan cannot diagnose impulsivity in an individual patient. The correlation supports the idea that addiction-related behavior is tied to measurable network organization, especially in systems that combine reward valuation and self-regulation.
- Not substance-specific only: Findings were not limited to one drug class.
- Not purely reward-based: Control, salience, memory, and thalamic relay connections were also involved.
- Not treatment-ready alone: Network maps need prospective validation before guiding stimulation or medication decisions.
Resting-State fMRI Cannot Separate Cause From Consequence
The review pooled cross-sectional imaging studies, so the findings cannot show whether connectivity differences existed before addiction, emerged during chronic use, reflected withdrawal or abstinence, or changed after recovery. Many original studies also excluded severe psychiatric comorbidity, which can limit real-world generalizability.
Age and sex balance differed between patient and control groups in some source studies. Substance use disorder is also shaped by trauma, environment, genetics, treatment access, and medical comorbidity, none of which can be reduced to one network diagram.
Seed-based meta-analysis adds another constraint. It depends on the seed regions and coordinates reported in source papers, so it can identify recurring locations but cannot recover every network feature that individual studies may have measured differently.
Resting-state scans are also indirect. They measure synchronized blood-oxygen-level fluctuations rather than dopamine release, craving, withdrawal intensity, or moment-to-moment choice behavior. Clinical translation needs studies that connect the maps to outcomes people and clinicians can observe.
Shared Brain Networks May Help Target Addiction Treatments
A recurring reward-control map could still help future treatment development. If certain circuits are repeatedly altered across substances, noninvasive brain stimulation, cognitive training, medications, or psychotherapy studies can test whether changing those circuits improves craving, impulsivity, or relapse risk.
The strongest clinical use will require longitudinal evidence. A useful next step would follow patients over treatment and recovery to see whether connectivity normalization predicts better outcomes or simply accompanies symptom improvement.
The review also gives treatment researchers a more specific vocabulary. Instead of treating substance use disorder as a single reward deficit, future trials can ask whether frontal inhibition, striatal habit circuitry, thalamic relay function, or emotion-memory pathways are the relevant target for a given intervention.
Trial design has to respect those circuit differences because stimulation targets and behavioral therapies are not interchangeable. A treatment meant to strengthen inhibitory control may need different markers than a treatment meant to reduce cue-reactive memory or stress-driven relapse in patients.
For now, the review is best read as a map of shared vulnerability systems. It narrows the set of circuits that deserve repeated testing, while leaving individual diagnosis and treatment selection to future prospective studies.
Citation: DOI: 10.1038/s41398-025-03396-2; Zhang et al; Common neural patterns of substance use disorder: a seed-based resting-state functional connectivity meta-analysis; Translational Psychiatry; 2025;15:190.
Study Design: Seed-based resting-state fMRI systematic review and meta-analysis.
Sample Size: 53 studies with 1,700 people with substance use disorder and 1,792 healthy controls.
Key Statistic: Reduced striatum-to-median-cingulate connectivity was negatively correlated with BIS-11 impulsivity scores.
Caveat: Cross-sectional source studies, substance-stage differences, and demographic imbalance limit individual-level interpretation.