TL;DR: A 2026 preprint in medRxiv linked atypical absence seizures in SYNGAP1-related developmental and epileptic encephalopathy (SYNGAP1-DEE) to higher caregiver-reported autistic behavior scores, while caregiver-reported peak seizure frequency did not show the same association.
Key Findings
- 337-person analytic cohort: Researchers analyzed 337 SYNGAP1 registry participants with complete epilepsy and behavior questionnaires.
- 259 epilepsy-positive participants: Epilepsy was reported in 259 people, making seizure type central to the analysis.
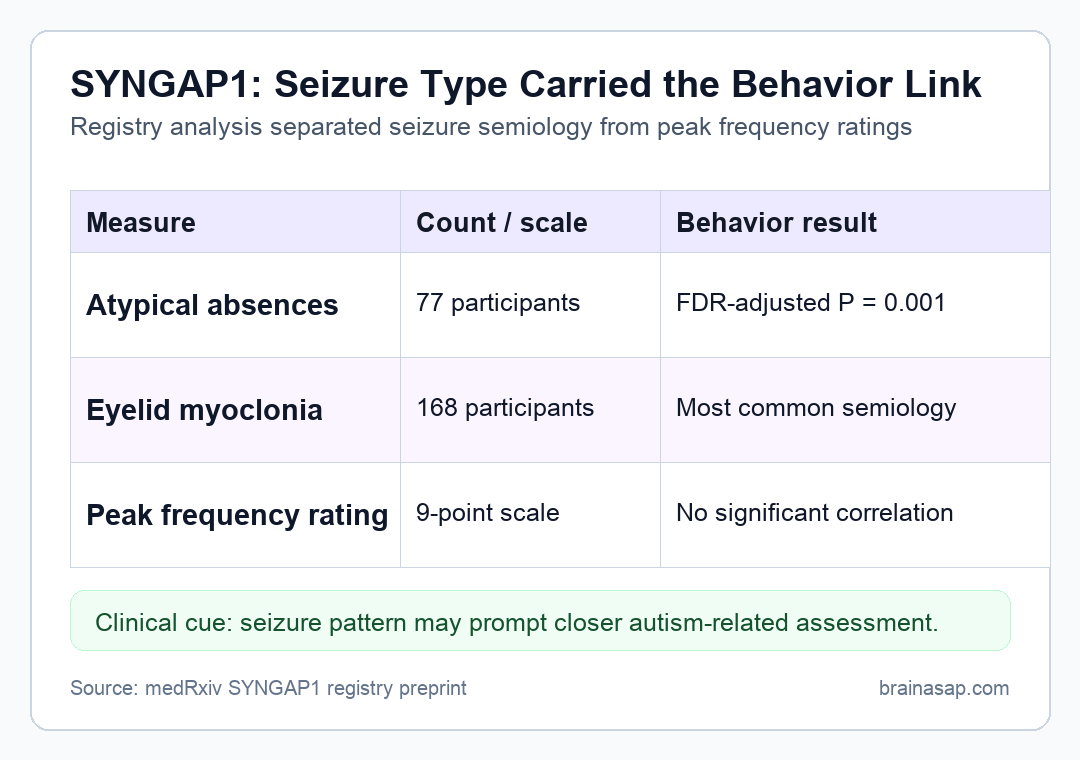
- Atypical absence signal: Atypical absences were reported in 77 participants and had the strongest association with higher caregiver-reported autistic behavior scores (FDR-adjusted P = 0.001).
- Eyelid myoclonia was common: Eyelid myoclonia affected 64.9% of the epilepsy-positive group, or 168 participants.
- Frequency did not track behavior: Peak seizure-frequency ratings were not significantly correlated with autistic behavior scores, including atypical absences (P = 0.744).
Source: medRxiv (2026) | Kiwull et al.
SYNGAP1-related developmental and epileptic encephalopathy (SYNGAP1-DEE) is a rare neurodevelopmental disorder in which pathogenic SYNGAP1 variants are often accompanied by epilepsy, intellectual disability, and autistic traits. The new analysis asked whether the kind of seizure mattered more than the reported number of seizures.
That distinction is clinically useful because families and clinicians often describe epilepsy burden by frequency. In this registry analysis, seizure semiology, meaning the observable seizure type or pattern, was more informative for caregiver-reported autistic behaviors.
Atypical Absence Seizures Had the Strongest SYNGAP1 Behavior Association
The main result involved atypical absences, a generalized seizure type often tied to thalamocortical networks. In the analytic cohort, atypical absences were reported in 77 participants.
Participants with atypical absences had higher caregiver-reported autistic behavior scores, with an FDR-adjusted P value of 0.001. FDR adjustment means the analysis corrected for multiple seizure-type comparisons to reduce false-positive findings.
- Typical absences: Reported in 70 participants and associated with higher behavior scores after correction (FDR-adjusted P = 0.018).
- Myoclonic-atonic seizures: Reported in 40 participants and also associated with higher behavior scores (FDR-adjusted P = 0.019).
- Atonic seizures: Reported in 72 participants and associated with higher behavior scores (FDR-adjusted P = 0.025).
The pattern points toward generalized seizure networks, not just any epilepsy history. Focal and tonic-clonic seizures showed weaker corrected associations in the abstracted results.
Seizure Frequency Ratings Did Not Explain the Autistic Behavior Scores
The analysis also tested peak seizure frequency using a 9-point caregiver-reported scale, ranging from once in a lifetime to several times per hour. This frequency measure did not show a detectable association with caregiver-reported autistic behavior scores.
For eyelid myoclonia, the frequency-behavior correlation had P = 0.096. For atypical absences, it had P = 0.744, far from a conventional statistical threshold.
- Seizure type: Which seizure semiologies were present?
- Peak frequency: How often did caregivers report the seizures at their historical peak?
- Behavior score: How high were caregiver-reported autistic behavior scores on the registry scale?
The pattern was not simply that more seizures meant higher autistic behavior scores. The reported seizure type had the clearer association.
The PATRE Registry Captured Caregiver-Reported Rare Epilepsy Data
Data came from the PATRE SYNGAP1 registry, a patient-centered rare-epilepsy registry connected to the EURAS project. Of 522 registered participants, 337 had complete data for both the epilepsy and behavior questionnaires used in this analysis.
Caregivers identified seizure types from a predefined list based on the 2017 International League Against Epilepsy classification. Autistic behaviors were measured with a caregiver-reported Likert scale from 1 to 5.
- Registry strength: Rare-disease registries can assemble larger cohorts than a single clinic usually can.
- Registry limit: Caregiver reports can contain recall error, classification uncertainty, or uneven missing data.
- Analysis boundary: Cross-sectional registry data can show associations but cannot prove that one seizure type causes autistic behaviors.
The analysis used Wilcoxon rank-sum tests for seizure-type comparisons and Spearman rank correlations for frequency ratings. Those methods match the ordinal, caregiver-reported nature of the data.
Eyelid Myoclonia Was Common but Atypical Absences Were More Specific
Eyelid myoclonia was the most common reported semiology, affecting 168 epilepsy-positive participants. It was also associated with higher caregiver-reported autistic behavior scores after correction.
Atypical absences were less common but statistically more robust in this analysis. That combination makes them a potential clinical flag rather than just another frequent seizure category.
- Common pattern: Eyelid myoclonia may help clinicians recognize the broader epilepsy phenotype in SYNGAP1-DEE.
- Stronger association: Atypical absences may point more specifically toward higher caregiver-reported autistic behavior burden.
- Network interpretation: The authors framed atypical absences as a generalized thalamocortical seizure-network marker.
That interpretation is plausible but should remain tied to the registry data. The study did not include EEG-confirmed seizure classification for every event or a longitudinal test of whether seizure pattern predicts later behavioral change.
SYNGAP1-DEE Care May Need More Than Seizure Counts
The clinical implication is straightforward: counting seizures alone may miss part of the neurodevelopmental picture in SYNGAP1-DEE. Specific seizure semiologies could help identify children who need more detailed autism-related assessment and support.
The finding also pushes against treating epilepsy as only present or absent in rare neurodevelopmental disorders. In this cohort, the kind of seizure mattered more than a caregiver-rated frequency score.
- Best-supported use: Treat atypical absences and related generalized semiologies as prompts for closer behavioral screening.
- What not to infer: Do not use the preprint to claim that reducing atypical absences will automatically lower autistic behavior scores.
- Next evidence step: Longitudinal data with clinician-confirmed seizure classification would clarify whether these patterns predict developmental trajectories.
For families, the result may help explain why children with similar seizure counts can have different developmental profiles. In SYNGAP1-DEE, seizure network pattern may be part of the clinical picture.
Citation: DOI: 10.64898/2026.04.19.26351217. Study authors et al. Kiwull et al. Beyond Seizure Burden: Seizure Semiology, but not Frequency, is Associated with Caregiver-Reported Autistic Behaviors in SYNGAP1-DEE. medRxiv . 2026.
Study Design: Retrospective cross-sectional registry analysis of caregiver-reported SYNGAP1 epilepsy and behavior data.
Sample Size: 337 analytic participants, including 259 with caregiver-reported epilepsy.
Key Statistic: Atypical absences were associated with higher caregiver-reported autistic behavior scores after correction (FDR-adjusted P = 0.001).
Caveat: The source was a preprint using caregiver-reported cross-sectional registry data, so causality and individual prognosis are not established.