TL;DR: A 2026 meta-analysis in European Journal of Psychotraumatology found that trauma cues increased substance craving in trauma-exposed people who use substances, and the strongest pathway ran through cue-triggered negative affect.
Key Findings
- 32 studies: Researchers synthesized trauma cue-reactivity studies from 21 unique datasets.
- Craving increased with trauma cues: Trauma reminders produced higher craving than baseline, neutral cues, and substance cues.
- Largest cue contrast: Trauma cues had a medium effect relative to neutral cues, with d = 0.526.
- Negative affect pathway: Trauma cues increased negative affect, and negative affect was linked to stronger substance craving.
- Clinical caution: Laboratory craving is not the same outcome as relapse, substance use frequency, or treatment response.
Source: European Journal of Psychotraumatology (2026) | DeGrace et al.
Trauma cues are reminders of traumatic experiences, such as images, sounds, memories, or personalized scripts that bring traumatic material back into attention.
For some people with substance use problems, those reminders do more than increase distress. They can also increase craving.
The new meta-analysis focused on the bridge between trauma reminders and substance craving. Researchers asked whether trauma cues reliably increased craving in trauma-exposed people who use substances, and whether negative affect helped explain the link.
Negative affect means distressing emotional states such as fear, sadness, anger, anxiety, or shame. In addiction research, those internal states can become cues themselves when substance use has repeatedly been paired with relief from distress.
Meta-Analysis Focused on Trauma Cue Reactivity
The paper analyzed experimental cue-reactivity procedures. In these studies, participants are exposed to a cue, then researchers measure craving or related emotional responses.
A cue can be neutral, substance-related, trauma-related, or part of a pre-cue baseline condition.
The review included 32 studies drawn from 21 unique datasets. Participants were trauma-exposed individuals who used substances, and many samples included people with post-traumatic stress disorder (PTSD), substance use disorder (SUD), or both.
- Study population: Across included studies, participants ranged from age 16 to 45, with a mean age of about 32 years.
- Sex distribution: The combined study samples were about 51% female.
- Clinical burden: In studies assessing diagnosis, an average of 56% of participants had PTSD and 87.7% had SUD.
This overlap is important because trauma cue reactivity is especially relevant when PTSD symptoms and substance use patterns converge. If distress relief becomes part of the reason a person uses substances, trauma reminders may become a powerful trigger for craving.
Trauma Cues Raised Craving Across Control Conditions
Trauma cues produced higher substance craving across the main control conditions. The effect was smaller relative to baseline, larger relative to neutral cues, and still present relative to substance cues.
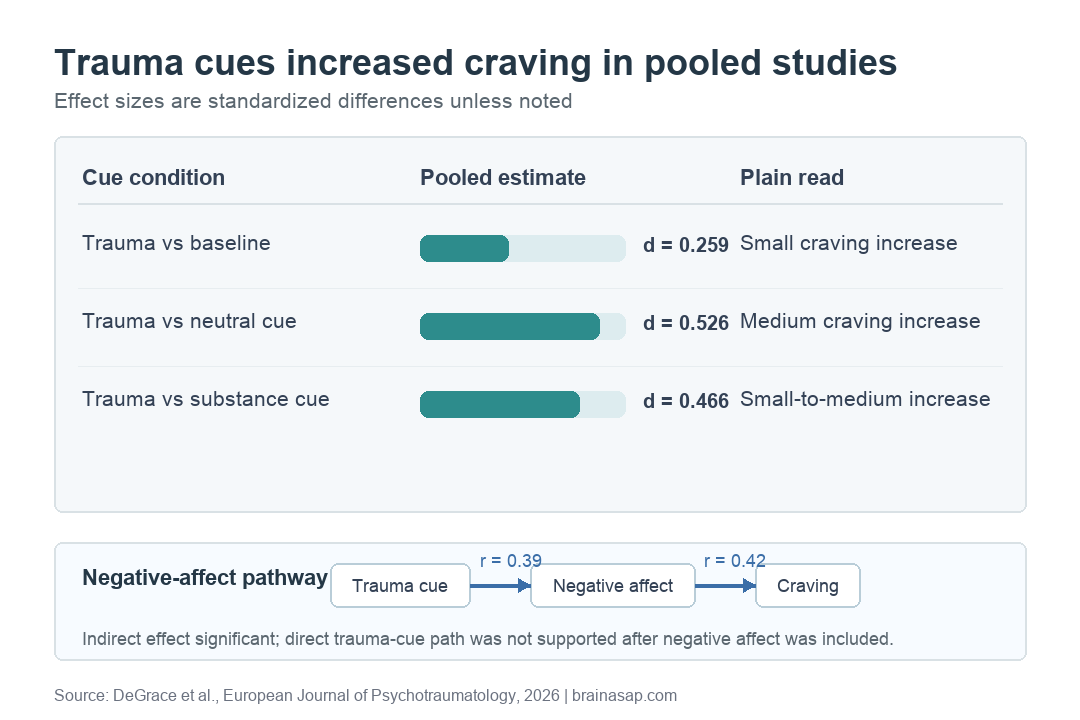
The trauma-versus-baseline effect was d = 0.259, which is a small effect. Trauma cues produced a medium effect relative to neutral cues, with d = 0.526.
Relative to substance cues, trauma cues still produced stronger craving, with d = 0.466.
The substance-cue result is clinically important. Substance cues are already known to raise craving. In this synthesis, trauma cues produced craving that was stronger than craving after substance cues.
- Baseline: Trauma reminders increased craving relative to a pre-cue or no-cue state.
- Neutral cues: Trauma reminders produced the largest estimated craving effect in the main analyses.
- Substance cues: Trauma reminders were not just another source of distress; they also outperformed substance cues as craving triggers in the pooled estimate.
Negative Affect Explained the Craving Pathway
The researchers also tested whether negative affect helped explain why trauma cues increased craving. They used two-stage meta-analytic structural equation modeling, a method that combines correlation patterns across studies to test an indirect pathway.
The modeled pathway was specific: trauma cue exposure was linked to higher negative affect, and higher negative affect was linked to stronger craving.
The trauma-to-negative-affect path was r = 0.39. The negative-affect-to-craving path was r = 0.42.
The indirect effect was statistically significant. After accounting for negative affect, the direct path from trauma cue exposure to craving was not supported.
The pooled data fit a distress-driven pathway better than a pathway where trauma reminders directly increased craving without the emotional response.
- Trauma cue: A reminder activates trauma-related emotional material.
- Negative affect: Distress rises after the cue.
- Craving: The distress state is associated with a stronger urge to use substances.
This fits self-medication and negative-reinforcement models of substance use. If using a substance has repeatedly reduced distress, then distress itself can become a learned craving trigger.
PTSD and Study Quality Moderators Were Unstable
The meta-analysis also looked for factors that changed the size of the trauma-cue effect. Some moderator signals appeared, but they were not consistent across every control condition.
For trauma cues relative to baseline, a higher percentage of participants with PTSD was linked to a stronger craving effect, but the estimate was marginal rather than clearly decisive. For trauma cues relative to neutral cues, cue-reactivity procedure type and study quality were associated with the effect size.
The paper treated those moderator findings cautiously. They depended on the control condition and, in some cases, on a small number of studies.
Moderator results are useful for designing better future experiments, but they are not strong enough to define clinical subgroups by themselves.
- PTSD burden: PTSD percentage may matter, but the baseline moderator signal was near the threshold for statistical significance.
- Procedure type: The way cues were delivered affected some estimates.
- Study quality: Higher-quality studies showed larger trauma-versus-neutral effects in one analysis.
Laboratory Craving Needs Clinical Caution
The findings support a clear mechanism: trauma reminders can increase craving, and negative affect appears to be an important route from the reminder to the urge. The meta-analysis still cannot prove that trauma cues cause relapse in daily life.
Laboratory craving is a useful outcome, but it is still a proxy. Real-world substance use depends on access, social context, withdrawal, treatment, coping skills, housing stability, sleep, stress, and many other factors.
The authors also noted limits in the evidence base. Many included studies came from North American samples, and craving and affect measures varied.
Some moderator tests had few studies behind them. Those limits matter when translating the findings into treatment planning.
The practical takeaway is still important. For people with trauma histories and substance use problems, treatment may need to address trauma reminders and distress regulation together.
Craving may spike not only around substances, but also around memories or cues that recreate emotional threat.
Citation: DOI: 10.1080/20008066.2026.2645996. DeGrace et al. When trauma triggers craving: meta-analytic evidence for the mediating role of negative affect among trauma-exposed individuals who use substances. European Journal of Psychotraumatology. 2026.
Study Design: Meta-analysis of trauma cue-reactivity studies, with two-stage meta-analytic structural equation modeling for the negative-affect pathway.
Sample Size: 32 studies from 21 unique datasets.
Key Statistic: Trauma cues increased craving relative to neutral cues with d = 0.526, and negative affect significantly mediated the trauma-cue-to-craving pathway.
Caveat: Laboratory craving, varied cue procedures, and mostly North American study samples limit direct claims about relapse or treatment response.





