TL;DR: A 2026 case study in Psychiatry and Clinical Neurosciences Reports described a 36-year-old man with treatment-resistant schizophrenia and focal epilepsy whose psychosis improved after slow clozapine titration, without worsening seizure frequency or severity during monitored hospitalization.
Key Findings
- Clozapine reached 250 mg/day: Treatment started at 6.25 mg and was titrated slowly over more than 3 months.
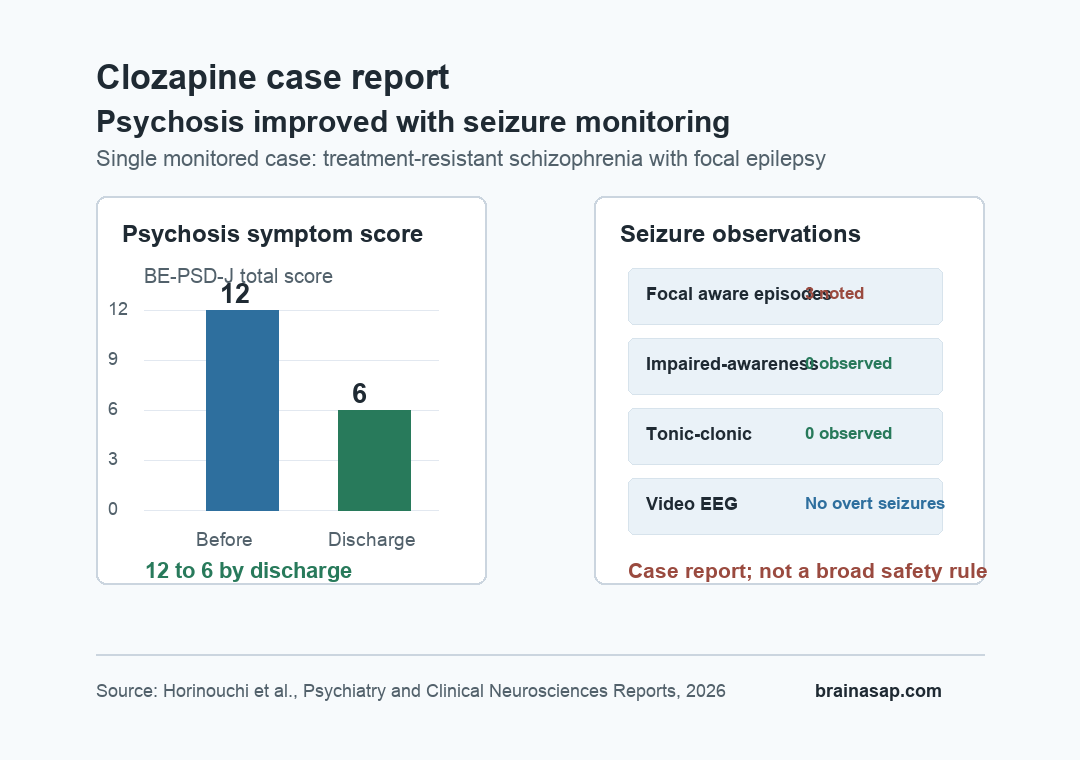
- Psychosis scores fell by half: The Brief Evaluation of Psychosis Symptom Domains Japanese version (BE-PSD-J), a psychosis-symptom rating scale, decreased from 12 to 6.
- Severe seizures did not return: During 5 months in the hospital, the patient had three focal aware seizure episodes but no focal impaired awareness seizures or focal to bilateral tonic-clonic seizures.
- EEG still mattered: Four-day video electroencephalography (EEG), a test that records brain electrical activity, found rare frontal spike-and-wave activity but no overt epileptic seizures.
- The evidence is still narrow: This is one carefully monitored case, not proof that clozapine is broadly safe for every patient with schizophrenia and epilepsy.
Source: Horinouchi et al. Psychiatry and Clinical Neurosciences Reports, 2026.
Clozapine is often the key medication for treatment-resistant schizophrenia, but epilepsy makes the decision harder. Clozapine can lower seizure threshold, and some prescribing systems list uncontrolled epilepsy as a contraindication or major warning.
This case report focused on a patient whose schizophrenia had not responded adequately to multiple antipsychotic drugs. He also had a long history of focal epilepsy, including earlier focal to bilateral tonic-clonic seizures.
The clinical question was not whether clozapine is risk-free. It was whether a carefully monitored start could improve psychosis without causing a meaningful seizure setback.
Slow Clozapine Titration Was Used Because Epilepsy Raised the Risk
The patient was a 36-year-old man with treatment-resistant schizophrenia and focal epilepsy. He had childhood-onset loss-of-consciousness episodes, later focal to bilateral tonic-clonic seizures, and evidence suggesting a frontal-lobe seizure focus.
Before clozapine, his psychiatric symptoms included auditory hallucinations, delusional mood, social withdrawal, and insomnia. Several antipsychotics had been tried without enough benefit, including:
- Olanzapine and quetiapine: Earlier treatment produced limited improvement.
- Aripiprazole, risperidone, brexpiprazole, lurasidone, and paliperidone: Sequential trials were also unsuccessful.
- Antiseizure treatment: Lamotrigine, valproic acid, and gabapentin were part of the admission regimen.
Clinicians judged the epilepsy as not uncontrolled because the most recent major seizure had occurred more than 2 years earlier, adherence was strong, and antiseizure medication levels were within therapeutic ranges. That distinction mattered: the report does not describe clozapine use in actively uncontrolled epilepsy.
Clozapine was started at 6.25 mg/day, lower than standard titration in many settings, and increased slowly. It took more than 3 months to reach 250 mg/day, with a measured clozapine plasma concentration of 449 ng/mL.
Psychosis Improved While Major Seizures Stayed Absent
By discharge, the patient’s psychotic symptoms had improved. The report measured this with the BE-PSD-J, a brief scale that rates psychosis symptom domains.
The total score moved from 12 before clozapine to 6 at discharge.
The patient’s delusional mood disappeared, and auditory hallucinations were subjectively reduced by about 30%. Side effects were present but manageable, including drowsiness, drooling, and constipation.
Seizure outcomes were monitored closely during the 5-month hospitalization. The patient had three focal aware seizure episodes, described as dizziness, but did not have the more disruptive seizure types that had been part of his earlier history.
- No focal impaired awareness seizures: These episodes involve impaired awareness and had occurred before admission.
- No focal to bilateral tonic-clonic seizures: The report did not observe return of the more severe convulsive seizure pattern during hospitalization.
- Antiseizure medications were unchanged: Valproic acid and lamotrigine levels remained stable during admission.
The researchers therefore categorized seizure status as no remarkable change rather than improved. That wording is important.
The case supports careful feasibility in one patient, not a claim that clozapine protects against seizures.
EEG Monitoring Found Rare Frontal Spikes But No Overt Seizures
EEG monitoring added a second safety layer. Before clozapine, routine EEG did not show definitive interictal epileptiform discharges, which are abnormal brain-wave patterns that can appear between seizures.
After the dose reached 250 mg/day, the team used 4 days of video EEG monitoring to look for seizures the patient might not notice. No epileptic seizures were detected, but rare frontal spike-and-wave activity appeared only three times over the 4-day recording.
The report treated that finding cautiously. Clozapine may have enhanced epileptic activity or activated the pre-existing seizure focus, even though the clinical seizure pattern did not worsen in a major way.
The practical tension is that symptom improvement occurred alongside a signal that still required neurological monitoring.
The authors also emphasized C-reactive protein (CRP), an inflammation marker. CRP does not directly measure seizure risk, but inflammation can raise clozapine concentrations by affecting drug metabolism.
In this case, CRP rose once to 4.19 mg/dL early in treatment, then remained mostly around 0-1.0 mg/dL during hospitalization.
Prior Case Reports Mostly Found Psychosis Improvement, But Seizure Risk Stayed Unpredictable
The paper also reviewed prior case reports of clozapine use in psychosis with comorbid epilepsy. Across 16 identified cases, psychotic symptoms improved in all cases.
Among the 12 cases with seizure outcome data, the seizure outcome was:
- Improved in 5 cases: Seizure control was described as better after clozapine in those reports.
- No remarkable change in 6 cases: Seizure status did not meaningfully worsen.
- Worsened in 1 case: Tonic-clonic seizures increased after clozapine despite prior seizure control.
Those case reports are encouraging but not definitive. They are selected clinical stories, and they do not estimate the true rate of seizure worsening.
The single worsened case also matters because it shows that seizure deterioration cannot be predicted from dose or antiseizure medication choice alone.
In the current case, several safeguards likely helped: stable antiseizure medication, slow clozapine titration, blood-level monitoring, CRP monitoring, standardized psychiatric and side-effect scales, and inpatient observation. Those safeguards are part of the finding, not background details.
This Case Supports Careful Monitoring, Not Routine Use in Uncontrolled Epilepsy
The most useful takeaway is narrow. A patient with treatment-resistant schizophrenia and relatively controlled focal epilepsy improved on clozapine when the drug was started slowly and monitored with both psychiatric and neurological measures.
Several boundaries keep the case from being overread:
- Single-patient evidence: One case cannot establish general safety or guide dosing for broad clinical practice.
- Controlled inpatient setting: The patient was monitored for months in a hospital, which is different from routine outpatient titration.
- Epilepsy was not uncontrolled: The report explicitly depended on low recent seizure frequency and stable antiseizure medication levels.
- EEG activity still appeared: Rare frontal spike-and-wave activity means neurological risk did not disappear.
For clinicians and patients, the case adds a concrete example of how clozapine can be considered when schizophrenia is treatment-resistant and epilepsy is present but not actively uncontrolled.
The decision still depends on individualized risk assessment, antiseizure treatment stability, slow titration, inflammatory monitoring, clozapine blood levels, and readiness to stop or slow dose escalation if warning signs appear.
Citation: DOI: 10.1002/pcn5.70330. Horinouchi et al. Clozapine for treatment-resistant schizophrenia with epilepsy: A case report. Psychiatry and Clinical Neurosciences Reports. 2026;5:e70330.
Study Design: Single-patient case report with literature review of prior clozapine use in psychosis with comorbid epilepsy.
Sample Size: One 36-year-old man with treatment-resistant schizophrenia and focal epilepsy; literature table summarized 16 cases.
Key Statistic: BE-PSD-J psychosis score decreased from 12 to 6; clozapine reached 250 mg/day with plasma concentration 449 ng/mL; no focal impaired awareness or focal to bilateral tonic-clonic seizures occurred during hospitalization.
Caveat: This is a carefully monitored case report, not evidence that clozapine is safe for uncontrolled epilepsy or for all patients with schizophrenia and seizure history.





