TL;DR: A 2026 medRxiv preprint found that serum hydrogen sulfide (H2S) levels, a blood measure tied to brain signaling and inflammation biology, were about 7.7-fold lower in drug-naive major depressive disorder patients than in matched controls.
Key Findings
- 100-person comparison: Researchers enrolled 50 drug-naive major depressive disorder patients and 50 age- and sex-matched healthy controls in eastern India.
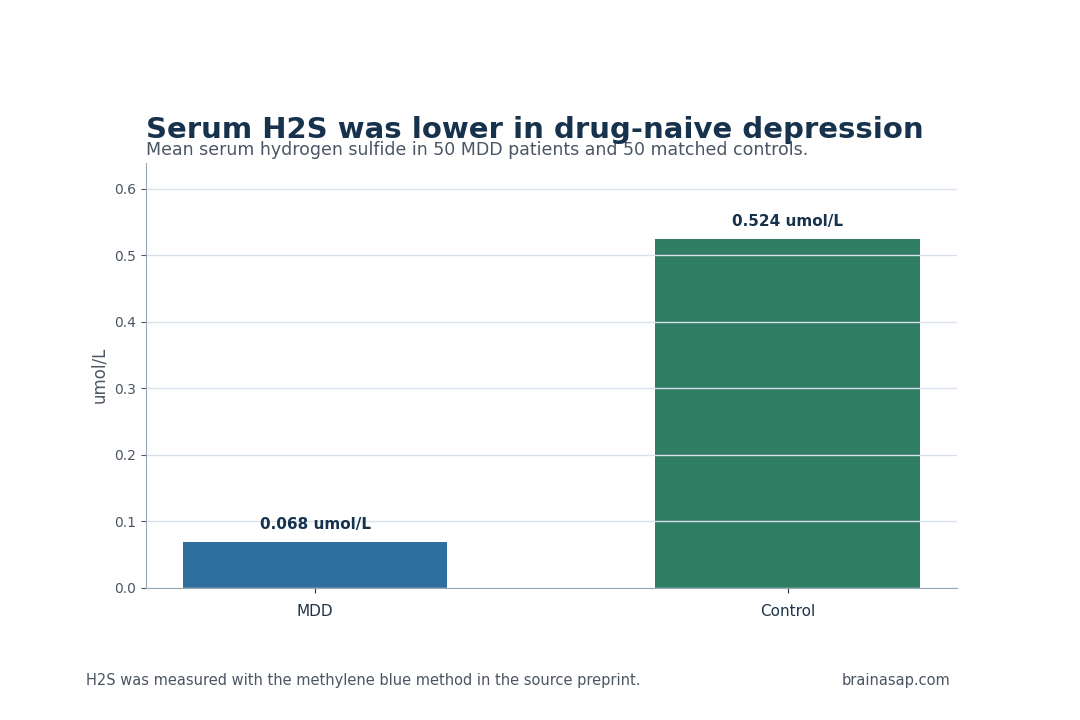
- 7.7-fold lower H2S: Mean serum hydrogen sulfide was 0.068 umol/L in depression versus 0.524 umol/L in controls.
- HAM-D-17 severity gap: Mean 17-item Hamilton Depression Rating Scale scores were 28.94 in depression and 3.96 in controls.
- Combined-cohort association: Across all participants, higher serum H2S was associated with lower depression severity, with R2 = 0.287.
- Within-MDD regression was weak: Inside the depression group alone, R2 was 0.061, consistent with a floor-effect or range restriction problem.
Source: medRxiv (2026) | North Bengal Medical College research team
Drug-Naive Depression Patients Had Much Lower Serum H2S Levels
Major depressive disorder is usually measured through symptoms, but the biology under those symptoms includes synaptic plasticity, inflammatory signaling, oxidative stress, and neurotrophic support. The source study tested whether a circulating gasotransmitter tied to those pathways differed between untreated patients and healthy controls.
The study focused on drug-naive patients because antidepressant exposure can complicate biomarker interpretation.
Researchers measured serum H2S in 50 people with DSM-5 major depressive disorder and 50 matched controls at a tertiary care center in West Bengal, India. Depression severity was measured with the 17-item Hamilton Depression Rating Scale (HAM-D-17), a clinician-rated symptom scale.
The group difference was large. Mean serum H2S level was 0.068 umol/L in the depression group versus 0.524 umol/L in healthy controls.
That is roughly a 7.7-fold reduction, and the group difference had p < 0.001.
Because participants were drug-naive, the study reduces one common source of biomarker confusion.
Antidepressants can alter sleep, appetite, inflammation, oxidative stress, and metabolic state, all of which can influence peripheral measurements. Starting before medication exposure gives the case-control contrast a cleaner interpretation.
HAM-D-17 Scores Were Higher When Serum H2S Levels Were Lower
Severity also moved in the expected direction across the whole sample. Mean HAM-D-17 score was 28.94 in the depression group, compared with 3.96 in controls.
When all participants were analyzed together, serum H2S showed a negative association with HAM-D-17 score: higher H2S aligned with lower depression severity.
The combined-cohort regression had R2 = 0.287, with the fitted equation y = 24.64 – 26.84x. H2S explained a measurable portion of symptom-score variation across the full case-control sample.
The finding does not prove that H2S alone can diagnose depression or that low H2S causes symptoms.
- Case-control contrast: Serum H2S levels were markedly lower in drug-naive depression than in controls.
- Severity scale: HAM-D-17 captured the symptom difference between the groups.
- Combined association: Lower serum H2S levels aligned with higher depression severity when cases and controls were pooled.
The within-group analyses are a guardrail. Inside the depression group alone, the regression was weak, with R2 = 0.061. Inside controls alone, it was much stronger, with R2 = 0.772.
That asymmetry suggests the biomarker may separate illness from health better than it grades severity among already-ill patients.
H2S Biology Connects Depression to Oxidative Stress and BDNF
The preprint frames H2S through several mechanisms that already appear in depression research. Preclinical work links H2S deficiency to synaptic plasticity, neuroinflammation, oxidative stress, and brain-derived neurotrophic factor signaling.
BDNF is a growth-factor system involved in neuronal survival, plasticity, and stress-related adaptation.
That biological context gives the serum measurement a plausible route into brain health, but it should be kept proportionate.
Serum H2S is a peripheral measurement. It can reflect systemic redox or inflammatory state, but it is not the same as directly measuring H2S signaling in specific brain regions.
The clinical value would depend on whether the blood measure behaves consistently across illness stages.
A marker that only separates untreated cases from healthy controls can help biology research, while a marker that changes with remission or relapse would be more useful for treatment monitoring.
The enzymes that generate H2S also matter for interpretation. Cystathionine beta-synthase and cystathionine gamma-lyase connect sulfur amino acid metabolism to redox biology.
If the finding replicates, the pathway would link depressive symptoms to metabolic stress rather than to a purely neurotransmitter-centered model.
The source also points toward a measurable clinical workflow. A future study would collect H2S at diagnosis, after treatment initiation, and after symptom remission.
If the blood measure rises as HAM-D-17 scores fall, it would support a state-sensitive biomarker role rather than a fixed vulnerability marker.
Researchers should also collect diet, sleep, inflammatory markers, and medical comorbidity at the same visits.
Those variables would help determine whether H2S is tracking depression biology itself or a broader health state that often accompanies depressive illness.
The Depression Biomarker Claim Is Strongest as a Case-Control Signal
The strongest use of these data is as a case-control biomarker observation. The depression group differed sharply from controls, and the participants had not yet been exposed to antidepressant medication.
That design avoids some of the medication-related ambiguity found in mixed treatment samples.
A diagnostic claim would require more work. A clinical biomarker would need replication in larger populations, testing against other psychiatric disorders, information on medical comorbidities, and evidence that the measurement performs well in real clinical settings.
It would also need stability data: does serum H2S change with treatment, remission, relapse, inflammation, diet, or sleep?
Specificity is the hardest biomarker issue. A low serum value can also appear in inflammatory illness, nutritional differences, chronic stress, or other psychiatric conditions.
Future studies should compare major depression with bipolar depression, anxiety disorders, inflammatory disorders, and medically ill controls before treating H2S as depression-specific.
Assay reliability also needs attention. A blood biomarker only helps clinicians if collection timing, sample handling, and laboratory method produce stable values across sites.
The methylene blue method is accessible, but multicenter validation would be needed before it can support routine psychiatric testing.
- Best-supported claim: Drug-naive MDD patients in this sample had lower serum H2S levels than matched controls.
- Open treatment endpoint: The source does not show whether H2S normalizes after antidepressant response.
- Open specificity endpoint: The comparison was healthy controls, not bipolar depression, anxiety disorders, inflammatory illness, or chronic pain.
Cross-Sectional H2S Results Need Longitudinal Testing
The main caveat is that the study was cross-sectional. It captured a single measurement window, so it cannot determine whether low H2S contributes to depression, follows depression, or reflects another biological state that travels with depression.
The sample was also modest, with 50 patients and 50 controls from one regional medical center.
The group difference is worth tracking because its magnitude was large and the patient group was drug-naive.
If future longitudinal studies show that serum H2S levels change with symptom improvement, relapse, or treatment choice, the CBS/CSE-H2S pathway would become more than a descriptive biomarker. It would become a testable target in depression biology.
Even a negative longitudinal result would be informative. If serum H2S levels stay low after remission, they can mark vulnerability or comorbid biology rather than current symptom burden.
For now, the direct conclusion is narrower: in this eastern India case-control study, serum H2S levels were substantially lower in untreated major depression, and lower values were associated with higher symptom scores when patients and controls were analyzed together.
Citation: DOI: 10.64898/2026.05.03.26352330; Reduced serum hydrogen sulfide levels in drug-naive major depressive disorder; medRxiv; 2026.
Study Design: Institution-based cross-sectional analytical case-control study.
Sample Size: 50 drug-naive MDD patients and 50 age- and sex-matched healthy controls.
Key Statistic: Mean serum H2S level was 0.068 umol/L in MDD versus 0.524 umol/L in controls.
Caveat: Cross-sectional serum data cannot establish cause, brain-region specificity, or treatment-response value.