TL;DR: A 2026 systematic review and meta-analysis posted to medRxiv found that gamma-frequency non-invasive brain stimulation was linked to symptom improvement in schizophrenia and depressive-symptom reduction in major depressive disorder, but the evidence was heterogeneous and still preprint-level.
Key Findings
- 56 controlled studies were included across schizophrenia, major depressive disorder, bipolar disorder, and autism spectrum disorder.
- Schizophrenia symptom scores improved versus controls, including total Positive and Negative Syndrome Scale (PANSS) scores and several symptom domains.
- Global cognition also improved in schizophrenia across 7 studies using cognitive batteries such as the MATRICS Consensus Cognitive Battery and MoCA, a brief cognitive screening test.
- Major depressive disorder showed a smaller effect on depressive symptoms, with high heterogeneity and publication-bias concerns.
- Bipolar disorder and autism evidence was not clearly positive in this review, so the result should not be generalized across all psychiatric conditions.
Source: Xu et al. in medRxiv, DOI: 10.64898/2026.04.10.26350641.
Gamma activity is a fast brain rhythm, usually discussed in the 30-100 Hz range. It is often linked to local circuit coordination, attention, sensory processing, and higher-order cognition.
The new review asked a practical treatment question: when non-invasive stimulation targets this gamma range, do clinical symptoms or cognitive outcomes actually improve in neuropsychiatric disorders?
Researchers searched 5 databases through April 2025 and pooled controlled trials of gamma neuromodulation. The included methods differed by stimulation type, frequency, duration, and session dose.
Some studies used transcranial alternating current stimulation, or tACS, which applies weak alternating electrical current through scalp electrodes. Others used theta-burst stimulation approaches such as intermittent theta-burst stimulation (iTBS) or continuous theta-burst stimulation, which are magnetic-stimulation protocols.
The review grouped the evidence into 4 diagnosis areas:
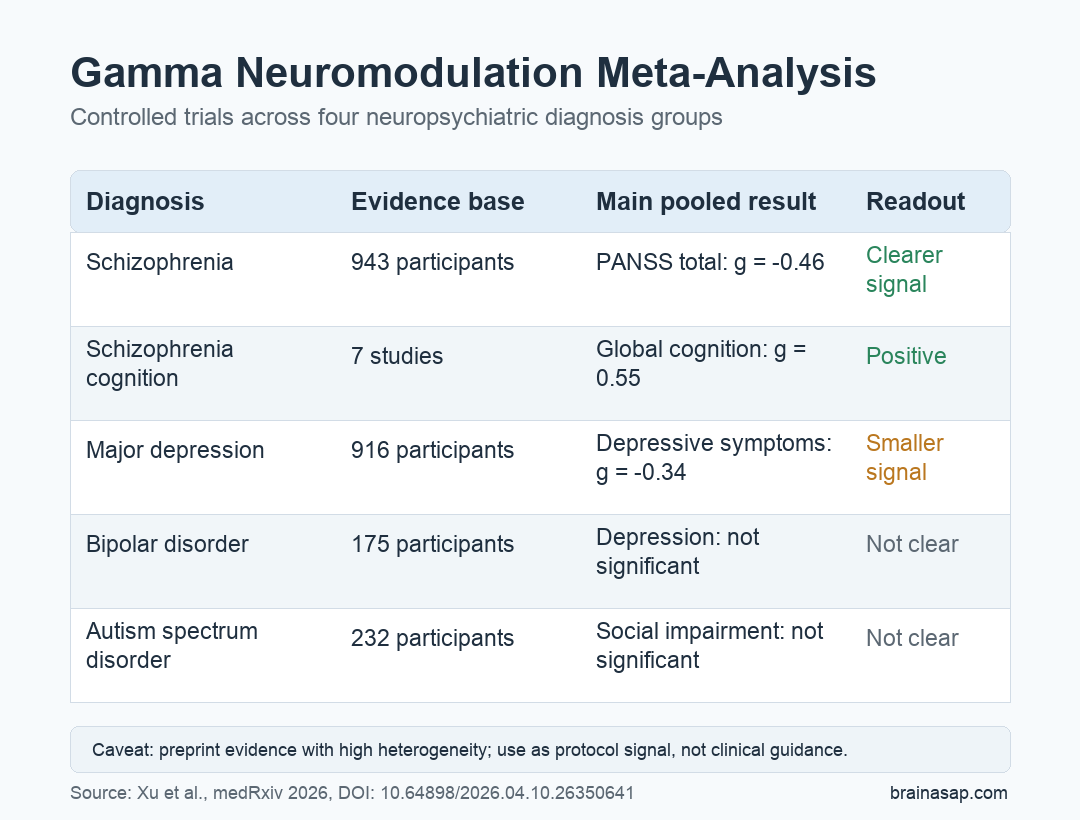
- Schizophrenia: 943 participants contributed to the pooled schizophrenia analyses.
- Major depressive disorder: 916 participants contributed to the pooled depression analyses.
- Bipolar disorder: 175 participants were represented, but the pooled clinical findings were not statistically clear.
- Autism spectrum disorder: 232 participants were represented, with no clear advantage over controls for social impairment.
The strongest pooled finding came from schizophrenia. Across 21 studies, gamma stimulation was associated with lower total PANSS scores than control conditions.
PANSS is the Positive and Negative Syndrome Scale, a clinician-rated schizophrenia scale that covers hallucinations or delusions, reduced motivation or social withdrawal, and broader symptom severity. Lower PANSS scores mean fewer or less severe symptoms.
Gamma Stimulation Showed Its Clearest Signal in Schizophrenia
For overall schizophrenia symptoms, the pooled effect was Hedges g = -0.46 versus controls. In this context, a negative value means symptom scores were lower in the active stimulation group.
The same effect size remained after researchers removed 8 outlier studies, which supports the same direction of effect across the sensitivity analysis. The limitation is that heterogeneity remained high, meaning the trials still differed substantially from one another.
The domain-level schizophrenia findings were also positive:
- Positive symptoms: 10 studies found a moderate reduction, with g = -0.60.
- Negative symptoms: twelve studies found a smaller but statistically significant reduction, with g = -0.37.
- Depressive symptoms: 8 studies found lower depressive symptoms, with g = -0.39.
- Anxious symptoms: 5 studies found lower anxiety symptoms, with g = -0.59.
These results do not prove that gamma stimulation is ready as a routine schizophrenia treatment. They show the pooled controlled-trial effect was not limited to one narrow symptom category.
Cognition was the other notable schizophrenia result. Across 7 studies, gamma stimulation improved global cognitive performance on tools such as the MATRICS Consensus Cognitive Battery, a schizophrenia-focused cognitive test battery, and the Montreal Cognitive Assessment (MoCA), a brief cognitive screening test.
The reported cognitive effect was g = 0.55. Here, a positive value means better cognitive scores in the active stimulation group.
50 Hz and Longer Treatment Looked More Promising
The review also examined whether protocol features changed the schizophrenia effect. Two moderators stood out: stimulation frequency and treatment duration.
For stimulation frequency, 50 Hz had the clearer overall effect in schizophrenia, while 30 Hz and 40 Hz did not show the same pooled strength in the subgroup analysis. For duration, protocols lasting 2-3 weeks or more had larger effects than shorter protocols.
The practical pattern was:
- 1-week or shorter protocols: little evidence of a useful pooled effect.
- 1 to 2 weeks: a smaller effect estimate.
- 2 to 3 weeks: a larger effect estimate, with g = -0.61.
- More than 3 weeks: a moderate effect estimate, with g = -0.50.
This duration gradient supports a cumulative-treatment interpretation rather than a single-session interpretation. It cannot identify an ideal protocol by itself, because the subgroup estimates still depend on a limited and uneven set of studies.
Depression Findings Were Smaller and Less Stable
Major depressive disorder showed a statistically significant but smaller effect. Across 23 studies, gamma stimulation was associated with lower depressive symptoms than control conditions, with g = -0.34.
After 9 statistical outliers were removed, the effect remained significant and stayed in the small range at g = -0.30. The same direction after outlier removal helps the depression finding, but the review also reported high heterogeneity.
The depression analysis had another caution: funnel-plot inspection and Egger’s test suggested possible publication bias. In ordinary terms, the published or available evidence may overrepresent positive findings.
Unlike schizophrenia, the depression subgroup analyses did not identify a clear moderator for stimulation modality, frequency, duration, or pulses per session. The review therefore supports a broad pooled effect, not a protocol-specific recommendation.
Bipolar and Autism Results Did Not Clear the Same Bar
The bipolar disorder and autism spectrum disorder analyses were more limited. In bipolar disorder, the pooled depressive-symptom estimate favored active gamma stimulation, but it was not statistically significant.
In autism spectrum disorder, the pooled social-impairment result also favored active stimulation, but it did not reach statistical significance. Other autism-relevant symptoms and cognitive outcomes had too few studies for full meta-analysis.
The diagnosis-specific interpretation is more accurate. The review found its clearest clinical effect in schizophrenia, a smaller depressive-symptom effect in major depressive disorder, and insufficient support for broad claims in bipolar disorder or autism.
Gamma rhythms are biologically broad, but the same stimulation protocol may not work across different disorders, symptom targets, and circuit problems.
The Main Limitation Is Trial Heterogeneity
The source is a preprint, so it has not completed peer review. Preprint status does not make the results unusable, but it raises the standard for caution.
The larger methodological issue is heterogeneity. Trials differed by diagnosis, stimulation method, frequency, session count, outcome scale, and symptom target.
High heterogeneity means the pooled average should not be read as one uniform treatment effect. It is better read as a map of where the evidence is strongest and where future trials need cleaner protocol testing.
Gamma stimulation is not a proven psychiatric treatment from this review alone. The narrower conclusion is that controlled trials now show a measurable pooled effect in schizophrenia and major depression, and the schizophrenia finding appears stronger when stimulation is closer to 50 Hz and delivered over multiple weeks.
The next step is not more broad enthusiasm. It is larger, well-controlled trials that test specific frequencies, stimulation methods, treatment durations, and symptom targets against credible sham controls.
Citation: DOI: 10.64898/2026.04.10.26350641. Xu et al. Gamma Neuromodulation Provides Therapeutic Potential in Neuropsychiatry: A Systematic Review and Meta-Analysis. medRxiv. 2026.
Study Design: Systematic review and meta-analysis of controlled gamma-frequency non-invasive brain stimulation trials.
Sample Size: 56 studies, including 943 schizophrenia participants and 916 major depressive disorder participants.
Key Statistic: Schizophrenia total symptom scores improved with gamma stimulation (k = 21, Hedges g = -0.46), while depressive symptoms in major depressive disorder improved with a smaller effect (k = 23, Hedges g = -0.34).
Caveat: This is a preprint with high heterogeneity across protocols, so the results should guide trial design rather than clinical use.