TL;DR: A 2026 case-series study in Indian Journal of Psychological Medicine reported rapid pain and symptom improvement after accelerated transcranial direct current stimulation in 4 of 5 patients with treatment-resistant bodily distress disorder.
Key Findings
- 5 BDD cases: The series included 5 patients with bodily distress disorder, a condition involving persistent distressing physical symptoms and high healthcare use.
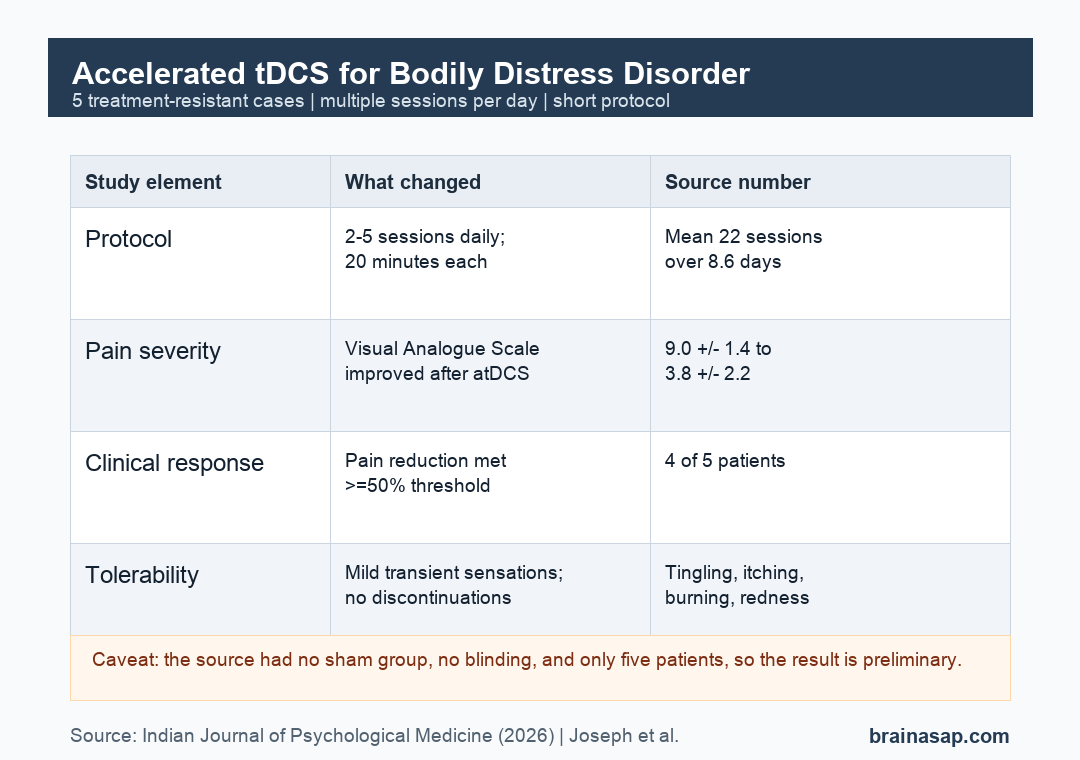
- Short accelerated protocol: Patients received 2 to 5 tDCS sessions per day, with a mean of 22 sessions delivered over 8.6 days.
- Pain scores decreased: Mean Visual Analogue Scale pain scores fell from 9.0 +/- 1.4 at baseline to 3.8 +/- 2.2 after treatment.
- 4 of 5 met response criteria: 4 patients achieved at least 50% pain reduction and at least a 2-point Clinical Global Impression-Severity improvement.
- No serious adverse events: Reported effects were mild and transient, including tingling, itching, burning, and skin redness.
Source: Indian Journal of Psychological Medicine (2026) | Joseph et al.
Bodily Distress Disorder Cases Were Treatment Resistant
Bodily distress disorder (BDD) involves persistent physical symptoms that cause marked distress, impairment, and repeated healthcare use. In older terminology, it overlaps with somatoform disorder.
The 5 patients in this case series had moderate to severe BDD, mostly with chronic pain symptoms. Illness duration ranged from 1 to 15 years, and 3 patients had already failed at least 2 medication trials.
Comorbidity was common. Some patients also had depressive disorder, anxiety or fear-related disorder, opioid dependence, sedative-hypnotic-anxiolytic dependence, nicotine dependence, or harmful use of non-psychoactive substances.
The study tested accelerated transcranial direct current stimulation (atDCS) as an add-on treatment. tDCS applies a weak electrical current through scalp electrodes to shift excitability in targeted brain networks.
All patients continued their existing medications during the stimulation course. The source is therefore most relevant as an adjunctive-treatment observation, not a test of atDCS as a stand-alone intervention.
Accelerated tDCS Compressed Treatment Into About 10 Days
Conventional tDCS protocols often require daily treatment over 4 to 6 weeks. This case series used an accelerated schedule to deliver multiple sessions per day and shorten the overall treatment period.
Each session used 2 mA stimulation for 20 minutes, with 30 seconds of ramp-up and ramp-down. Sessions were separated by about 1 to 2 hours.
The protocol varied by clinical profile:
- Motor cortex target: 4 patients received anodal stimulation over C3, corresponding to the left primary motor cortex, with the cathode over FP2.
- Prefrontal target: 1 patient with prominent anxiety and nonspecific pain received bilateral dorsolateral prefrontal cortex stimulation, with F3 as anode and F4 as cathode.
- Session burden: patients received 20 to 25 total sessions, with a mean of 22 +/- 2.7 sessions.
The motor-cortex target was based on pain-modulation work. Anodal tDCS over the left primary motor cortex has been studied for chronic pain and may influence thalamic activity and descending pain-control networks.
The prefrontal target in 1 patient reflected a different clinical presentation, with prominent anxiety and nonspecific pain. That variation is clinically understandable, but it makes the case series harder to interpret as a single standardized protocol.
Pain Scores Improved in 4 of 5 Patients
The primary outcome was daily pain severity on the Visual Analogue Scale (VAS), a 0-to-10 pain rating. Mean VAS scores decreased from 9.0 +/- 1.4 at baseline to 3.8 +/- 2.2 after treatment.
4 patients met the pain-response threshold of at least 50% reduction. The 1 nonresponder had comorbid substance use disorders, which the researchers noted can interact with somatic symptoms and complicate treatment response.
Global severity also improved. Mean Clinical Global Impression-Severity scores decreased from 6.8 +/- 0.5 to 3.4 +/- 0.9, and the same 4 patients met the response criterion of at least a 2-point reduction.
Additional symptom scales were used only when clinically relevant, so they cannot be pooled across all 5 patients. Still, the available scale results moved in the same general direction:
- Somatic symptoms: among 3 patients assessed with SASS, 2 showed substantial reductions of 44.7% and 77.3%.
- Depression: 2 patients with comorbid depression had Hamilton Depression Rating Scale reductions of 58.6% and 65%.
- Anxiety: the patient assessed with the Hamilton Anxiety Rating Scale had a 50% reduction.
Side Effects Were Mild and Transient
All patients completed the accelerated tDCS course. The source reported no serious adverse events and no treatment discontinuations.
Adverse effects were the kinds commonly monitored during tDCS:
- Tingling and itching: these were reported across multiple cases.
- Burning sensation: some patients reported transient burning during or around stimulation.
- Skin redness: 1 patient had skin redness, with no serious complication reported.
Tolerability is important because accelerated protocols increase the number of daily sessions. A short schedule is only useful if patients can realistically complete it without major discomfort or safety problems.
The Case Series Supports Feasibility, Not Proof
The main value of this report is feasibility. A multi-session daily atDCS schedule was deliverable in a clinical setting, and 4 of 5 patients had rapid symptom improvement.
The limits are just as important. There was no sham group, no randomization, no blinding, and only 5 patients.
Placebo effects, expectation, medication changes, regression toward the mean, or ordinary symptom fluctuation cannot be ruled out.
Patient and protocol differences also complicate interpretation. Most patients received left motor-cortex stimulation, but 1 received prefrontal stimulation, and not every patient completed every symptom scale.
For clinical research, the next step is straightforward: larger randomized trials with sham stimulation, consistent outcome measures, and longer follow-up. Until then, accelerated tDCS for bodily distress disorder should be treated as preliminary, not an established treatment.
Citation: DOI: 10.1177/02537176261442676. Joseph et al. Accelerated Transcranial Direct Current Stimulation as an Adjunctive Treatment for Rapid Symptom Relief in Bodily Distress Disorder: A Case Series. Indian Journal of Psychological Medicine. 2026;XX:1-4.
Study Design: 5-patient uncontrolled case series of accelerated tDCS as adjunctive treatment for bodily distress disorder.
Sample Size: 5 patients with moderate to severe bodily distress disorder and chronic pain symptoms.
Key Statistic: Mean VAS pain scores decreased from 9.0 +/- 1.4 to 3.8 +/- 2.2, and 4 of 5 patients achieved at least 50% pain reduction.
Caveat: The study had no sham-control group, blinding, randomization, or long-term follow-up.





