TL;DR: A 2026 sham-controlled study in BMC Psychiatry found that one 15-minute session of 1.5 mA anodal transcranial direct current stimulation (tDCS) over the right dorsolateral prefrontal cortex did not improve visuospatial or verbal working memory in clinically stable schizophrenia patients.
Key Findings
- 27 schizophrenia patients: The final analysis included 14 men and 13 women with clinically stable schizophrenia on stable antipsychotic regimens.
- Single-session tDCS: Active stimulation used 1.5 mA anodal tDCS for 15 minutes over the right dorsolateral prefrontal cortex (rDLPFC), with the cathode on the left cheek.
- No broad working-memory gain: Session-by-time interactions were not significant for CBT Forward, CBT Forward with Interference, CBT Backward with Interference, or Digit Span.
- CBT Backward was not a clear benefit: CBT Backward showed an interaction (F(1,26) = 6.011, p = 0.021), but post-hoc tests found no significant pre-post change within active or sham sessions.
- Baseline ability did not explain response: Linear mixed-effects models found no significant Session x Time x Baseline interactions across all tasks, with p values above 0.113.
Source: BMC Psychiatry (2026) | Ke et al.
Right DLPFC tDCS Was Tested for Schizophrenia Working Memory
Schizophrenia often includes cognitive deficits that are only partly addressed by antipsychotic medication. Working memory is one of the domains most closely tied to daily functioning.
The study tested whether transcranial direct current stimulation (tDCS), a noninvasive brain-stimulation method that applies weak electrical current through scalp electrodes, could acutely improve working memory.
The target was the right dorsolateral prefrontal cortex (rDLPFC), a frontal brain region involved in executive control and working-memory tasks. Prior work had suggested that stimulation effects might depend on baseline cognitive performance.
Researchers therefore asked two questions: did one stimulation session improve working memory compared with sham, and did lower baseline performance predict a larger response?
- Clinical group: 27 clinically stable schizophrenia patients, after one enrolled participant was excluded for not understanding task instructions.
- Medication stability: participants had stable antipsychotic treatment for at least 12 weeks and no acute psychiatric hospitalization in the prior 6 months.
- Trial design: randomized, sham-controlled, within-subject crossover, meaning each participant received active and sham sessions.
One 15-Minute tDCS Session Used 1.5 mA Current
The active session delivered 1.5 mA anodal tDCS for 15 minutes. The anode was placed over F4, the right-DLPFC location in the international 10-20 EEG system, and the cathode was placed on the left cheek.
The sham session used the same electrode placement and brief ramp-up/ramp-down sensation, but it did not provide sustained stimulation. Sessions were separated by at least 24 hours, and session order was counterbalanced.
Working memory was tested immediately before and after each session. The visuospatial task was a computerized Corsi Block-Tapping (CBT) battery, where participants recalled flashing block sequences.
The study used five working-memory outcomes:
- CBT Forward: recall the block sequence in the same order.
- CBT Backward: recall the block sequence in reverse order.
- Forward with interference: perform a motor interference task during retention, then recall forward.
- Backward with interference: perform interference, then recall backward.
- Digit Span Forward: hear digits and repeat them in order as a verbal working-memory measure.
Most Working-Memory Tasks Did Not Separate Active tDCS From Sham
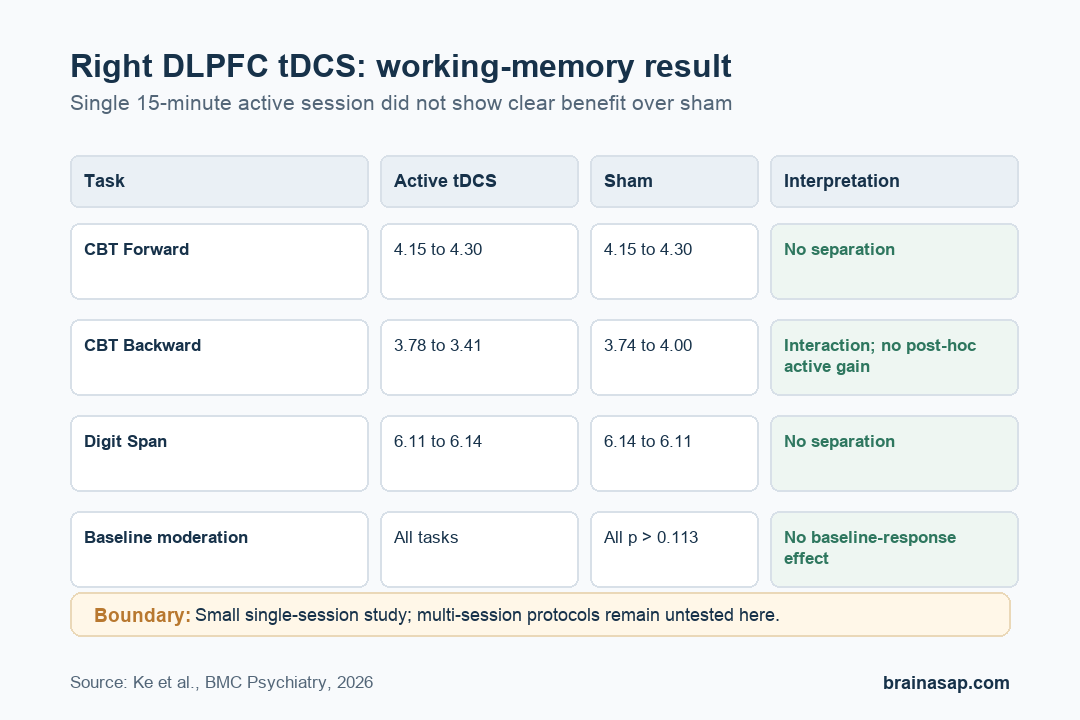
The main analysis looked for Session x Time interactions, meaning whether pre-to-post change differed between active tDCS and sham. Most tasks showed no significant interaction.
CBT Forward scores moved from 4.15 to 4.30 after active stimulation and from 4.15 to 4.30 after sham. Digit Span Forward was similarly flat: 6.11 to 6.14 after active stimulation and 6.14 to 6.11 after sham.
One task, CBT Backward, produced a significant interaction, with F(1,26) = 6.011 and p = 0.021. But the pattern did not support a clean treatment gain.
In CBT Backward, active-session mean scores decreased from 3.78 to 3.41, while sham-session scores increased from 3.74 to 4.00. Bonferroni-corrected post-hoc tests found no significant pre-post change within the active session or the sham session.
- Active CBT Backward: post-hoc p = 0.343 for the pre-post change.
- Sham CBT Backward: post-hoc p = 1.000 for the pre-post change.
- Clinical reading: the interaction was not evidence that active tDCS improved backward visuospatial span.
Lower Baseline Performance Did Not Predict Better tDCS Response
The researchers also tested whether participants with lower baseline visuospatial working memory would benefit more. Starting cognitive capacity was treated as a possible moderator of stimulation response.
Participants were split into low- and high-performing groups based on baseline CBT scores. The lower-performing group had lower full IQ, working-memory, Montreal Cognitive Assessment (MoCA) screening, and digit-span scores, but did not differ from the higher-performing group in right-DLPFC volume or resting functional connectivity.
Three-way ANOVA models found no significant Session x Time x Baseline Group interactions. Linear mixed-effects models treated baseline performance as a continuous moderator and reached the same conclusion.
For the continuous moderator models, all task p values were above 0.113. CBT Forward had p = 0.899, CBT Backward p = 0.121, Forward with Interference p = 0.113, Backward with Interference p = 0.239, and Digit Span p = 0.715.
The null moderation result suggests that the single-session protocol was not rescued by selecting participants with poorer baseline working memory.
Single-Target Brain Stimulation May Be Too Limited for Schizophrenia Cognition
The negative result does not rule out all tDCS approaches for schizophrenia cognition. It is specific to a single-session, single-target, offline testing protocol in a small stable outpatient sample.
The planned recruitment target had been 40 participants, but the final sample was 27 because of COVID-19-related logistical constraints. The study was powered for large effects, not the smaller or moderate effects often reported in recent tDCS meta-analyses.
The discussion framed schizophrenia working-memory deficits as distributed network dysfunction rather than a simple right-DLPFC deficit. Multi-session, network-based, or task-coupled protocols remain plausible next tests.
- Protocol limit: one 15-minute session may be too brief to shift cognition.
- Target limit: rDLPFC stimulation alone may not address broader frontoparietal and temporal network problems.
- Measurement limit: offline pre-post tasks may miss state-dependent effects during stimulation or training.
For now, the result argues against expecting immediate working-memory improvement from this exact right-DLPFC tDCS setup in stable schizophrenia.
Citation: DOI: 10.1186/s12888-026-08107-9. Ke et al. Anodal tDCS over right DLPFC does not improve visuospatial working memory in schizophrenia: a single-session, sham-controlled study. BMC Psychiatry. 2026.
Study Design: Randomized sham-controlled within-subject crossover brain-stimulation study.
Sample Size: 27 clinically stable schizophrenia patients.
Key Statistic: No significant Session x Time x Baseline interaction across working-memory tasks in linear mixed-effects models; all p values were above 0.113.
Caveat: Small sample and single-session protocol; findings do not rule out multi-session or network-based stimulation approaches.