TL;DR: A 2026 study in European Archives of Psychiatry and Clinical Neuroscience of 755 Korean adults with mood disorders found that three distinct childhood ADHD traits each tracked with different adult clinical features, suggesting ADHD’s influence on mood-disorder presentation is dimension-specific rather than uniform.
Key Findings
- Mood-disorder profiles split by ADHD trait: Researchers analyzed 755 adults — 287 patients with major depressive disorder and 468 with bipolar disorder — with retrospective childhood ADHD measured by the 25-item Wender Utah Rating Scale (WURS-25), a validated adult self-report of childhood attention and impulsivity symptoms.
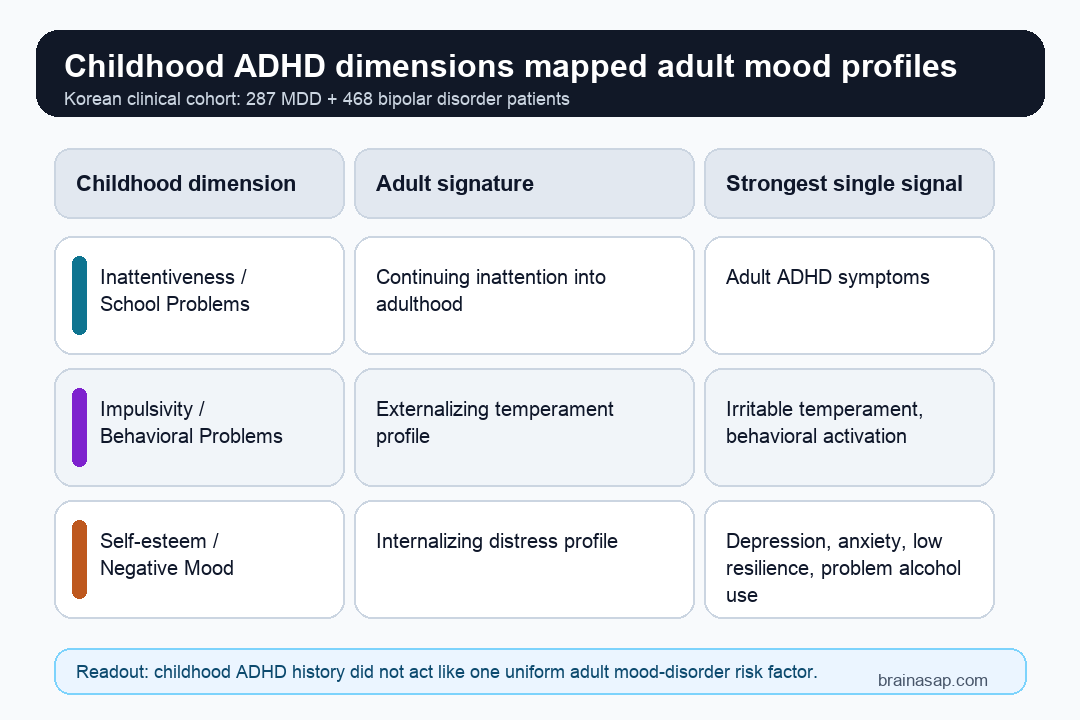
- Three childhood ADHD dimensions were tracked: The WURS-25 separates into Inattentiveness/School Problems, Impulsivity/Behavioral Problems, and Self-esteem/Negative Mood. Each dimension showed a distinct adult profile.
- Self-esteem/Negative Mood predicted internalizing problems: Higher scores on this dimension uniquely predicted greater adult depression and anxiety symptoms, higher behavioral inhibition, higher interpersonal sensitivity, lower resilience, and problematic alcohol use.
- Inattentiveness/School Problems best predicted adult ADHD: Across all three childhood dimensions, the inattention factor was the strongest and most consistent predictor of adult ADHD symptoms — the most expected finding, but worth measuring directly.
- Impulsivity/Behavioral selectively linked to externalizing traits: This dimension tracked with irritable temperament, behavioral activation, and (unexpectedly) lower interpersonal sensitivity — a pattern that does not generalize from the other two dimensions.
Source: European Archives of Psychiatry and Clinical Neuroscience (2026) | Jwa et al.
Childhood ADHD is widely understood to persist into adulthood in many cases, and the overlap with adult mood disorders is well documented.
What is less clear is whether childhood ADHD acts as one undifferentiated risk factor for adult psychiatric problems or whether different childhood ADHD components carry different adult signatures.
Clinical context: Splitting childhood ADHD into separate dimensions matters because adult mood-disorder care depends on whether attention, impulsivity, or early negative mood was the dominant childhood pattern.
Adults with bipolar disorder or major depression often carry residual or unrecognized ADHD features. The overlap creates real diagnostic problems because inattention and impulsivity can look similar across ADHD, mood episodes, and emotion dysregulation.
Stimulant prescribing in bipolar disorder is cautious for exactly this reason: raising dopaminergic activity in a patient prone to mania is risky.
If childhood ADHD is one broad construct, then any childhood-ADHD-positive mood patient should be treated similarly. If it is several distinct dimensions, the patient’s specific childhood profile may carry different prognostic and treatment implications.
The Jwa study set up that comparison directly using the WURS-25, a retrospective adult instrument that has shown reasonable validity for recalling childhood ADHD-related features in clinical mood populations.
The WURS-25 separates into three factors that consistently emerge in cross-cultural validation work:
- Inattentiveness/School Problems: Difficulty paying attention, school failure, organization problems — the classic inattentive presentation.
- Impulsivity/Behavioral Problems: Acting before thinking, fighting, getting in trouble — the externalizing presentation.
- Self-esteem/Negative Mood: Low self-worth, sadness, social difficulty — an emotional-distress dimension often dropped from neurodevelopmental ADHD frameworks but recurring in retrospective measures.
755 Mood-Disorder Adults, Three Childhood Dimensions, Many Adult Variables
The sample combined 287 adults with major depressive disorder and 468 adults with bipolar disorder, all assessed at a Korean psychiatric center. Participants completed the WURS-25 along with a broad battery of adult variables:
- Mood and anxiety symptoms: Depression severity, anxiety severity, current mood state.
- Affective temperament: Cyclothymic, depressive, irritable, hyperthymic, and anxious temperament scales.
- Emotional instability: Mood instability ratings.
- Adult ADHD symptoms: Self-report and clinical ratings of current attention and impulsivity.
- Emotion regulation: Cognitive reappraisal and expressive suppression strategies.
- Childhood trauma: Childhood Trauma Questionnaire subscales.
- Interpersonal sensitivity, resilience, and problematic alcohol use: Standardized scales.
Researchers first ran partial correlations to identify initial associations between each childhood ADHD trait and each adult variable, then ran path analysis to look at how those associations held up when modeled simultaneously.
Multigroup structural equation modeling tested whether associations differed between MDD and bipolar patients and between men and women.
The Strongest Adult Associations Were Mood Instability, Trauma, and Adult ADHD
Across all three childhood ADHD dimensions, the strongest adult correlates were:
- Trait mood instability: Higher childhood ADHD totals tracked with more adult mood instability.
- Childhood trauma exposure: Childhood ADHD was associated with higher reported childhood trauma scores, replicating a pattern seen in earlier cohorts.
- Adult ADHD symptoms: The retrospective childhood report correlated with current ADHD symptoms — expected but a useful internal validity check.
- Interpersonal sensitivity: Higher childhood ADHD totals tracked with more adult interpersonal sensitivity, particularly through the Self-esteem/Negative Mood dimension.
Among affective temperaments, depressive temperament showed the strongest association with childhood ADHD totals. Hyperthymic temperament — the energetic, optimistic, sociable profile — showed the weakest.
Emotion regulation skills had only minimal associations across the board, a clinically relevant null because emotion regulation has been a central target in adult ADHD-mood interventions.
Self-esteem/Negative Mood Was the Internalizing Track
The most clinically distinct dimension was Self-esteem/Negative Mood. Higher childhood scores on this factor uniquely predicted a cluster of adult internalizing problems:
- More adult depressive symptoms.
- More adult anxiety symptoms.
- Higher behavioral inhibition — a temperament marker of avoidance under uncertainty.
- Higher interpersonal sensitivity.
- Lower resilience.
- Higher rates of problematic alcohol use.
This is the dimension most often dropped from neurodevelopmental ADHD frameworks because it does not map onto inattention or impulsivity.
The Jwa results suggest it carries unique adult prognostic information in mood-disorder populations and may flag patients with a particular vulnerability to internalizing problems on top of their mood diagnosis.
Impulsivity/Behavioral Was the Externalizing Track
The Impulsivity/Behavioral Problems dimension mapped to a different profile:
- Irritable temperament: The temperament most often linked to mixed-state and treatment-resistant presentations.
- Higher behavioral activation: A temperament-level approach-motivation marker.
- Lower interpersonal sensitivity: The opposite direction from Self-esteem/Negative Mood, which is the clearest cross-dimension contrast in the paper.
The opposing direction on interpersonal sensitivity suggests that patients with high childhood impulsivity but low childhood self-esteem problems may look very different in the clinic from patients with the reverse pattern, even if their adult mood-disorder diagnosis is identical.
Why “ADHD-Plus-Mood” Should Probably Be Broken Down
For clinicians, the implication is direct. When a patient with bipolar disorder or major depression also screens positive for childhood ADHD, asking which ADHD features dominated childhood may shape adult care:
- Self-esteem/Negative Mood dominant: Watch for internalizing comorbidity, alcohol use, low resilience, and interpersonal-sensitivity-driven distress.
- Inattentiveness/School Problems dominant: Likely the patient with persistent adult ADHD symptoms; standard adult-ADHD assessment and treatment is most directly relevant.
- Impulsivity/Behavioral Problems dominant: Watch for irritable mood states and high behavioral activation, with the awareness that lower interpersonal sensitivity may make engagement strategies different.
The multigroup SEM finding that associations did not differ between MDD and bipolar patients or between men and women is reassuring for the dimension-specific framework.
The three-factor structure is doing similar work across diagnostic and sex boundaries, suggesting that the clinical implications generalize within mood-disorder populations rather than being trapped in one diagnostic category.
Retrospective Self-Report and Cross-Sectional Design Are Real Limits
Several constraints should keep interpretation careful:
- Retrospective childhood report: The WURS-25 asks adults to recall childhood symptoms. Recall validity is reasonable in published validation work but is not equivalent to prospective childhood diagnosis.
- Single-country sample: All 755 patients came from a Korean psychiatric center. Generalization to other populations needs separate confirmation.
- Cross-sectional design: Adult variables and childhood retrospective report were measured at the same visit. The directionality between childhood ADHD dimensions and adult profiles cannot be confirmed without prospective childhood-to-adult follow-up.
- Path analysis is not causal: SEM identifies which paths fit the data but cannot rule out unmeasured common causes — for example, shared early-life adversity that drives both childhood ADHD traits and adult mood-disorder severity.
This study is best read as a clinical-phenotyping framework rather than a causal model. It says that lumping all “ADHD-plus-mood” patients together loses information, and that asking about which childhood features dominated may add real prognostic detail to the adult workup.
Citation: DOI: 10.1007/s00406-026-02251-9. Jwa et al. Retrospective childhood attention-deficit/hyperactivity disorder traits and their differential associations with mood disorder presentations in adulthood. European Archives of Psychiatry and Clinical Neuroscience. 2026.
Study Design: Cross-sectional clinical cohort with retrospective childhood ADHD measurement (WURS-25), partial correlation and path analysis, and multigroup structural equation modeling.
Sample Size: 755 Korean adults with mood disorders: 287 with major depressive disorder and 468 with bipolar disorder.
Key Statistic: Three WURS-25 childhood ADHD dimensions each predicted distinct adult clinical profiles, with no significant differences between MDD and bipolar groups or between sexes.
Caveat: Cross-sectional design with retrospective childhood self-report; causal direction between childhood ADHD dimensions and adult profiles cannot be established.