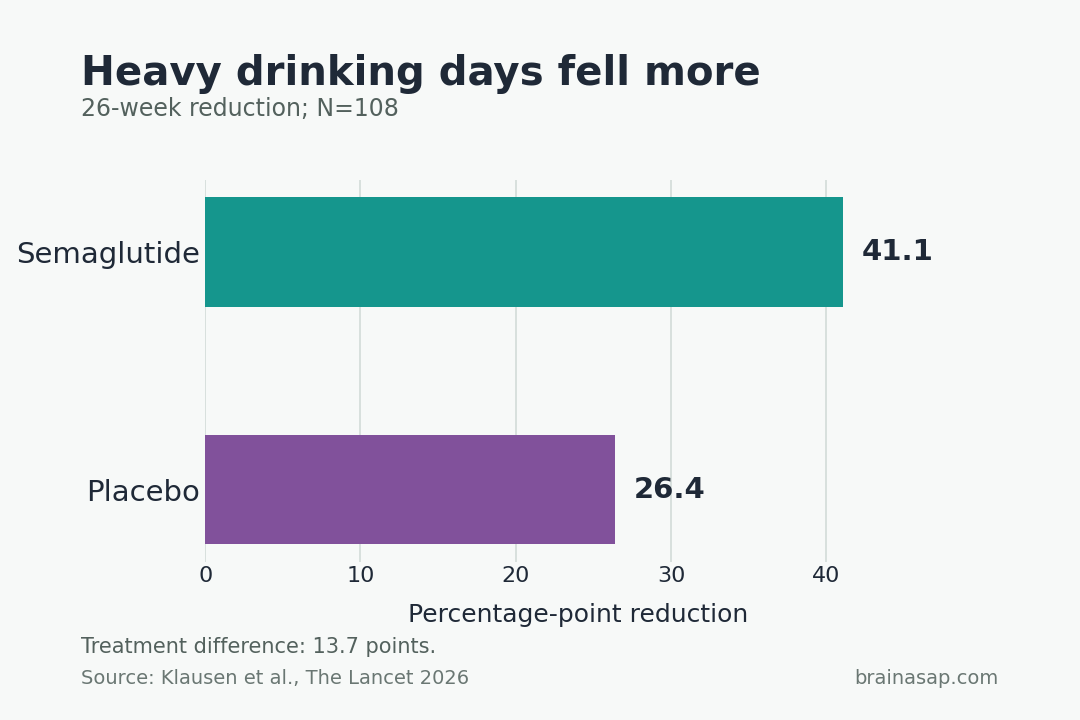
TL;DR: A 2026 randomized double-blind placebo-controlled trial in The Lancet (N=108 adults with both moderate-to-severe alcohol use disorder and obesity) found that 26 weeks of once-weekly 2.4 mg semaglutide reduced heavy drinking days by 41.1 percentage points compared with a 26.4-point reduction on placebo — a 13.7-point treatment difference, with parallel drops in alcohol craving, total volume consumed, and an objective blood biomarker of recent drinking.
Key Findings
- 13.7-point treatment difference in heavy drinking days: Semaglutide reduced heavy drinking days by 41.1 percentage points over 26 weeks; placebo reduced them by 26.4 percentage points. The 13.7-point gap is the primary efficacy result.
- Number needed to treat = 4.3: Only 4.3 patients had to receive semaglutide for one to achieve a strong outcome — below the typical NNT of 7+ for currently approved alcohol use disorder medications.
- Objective blood biomarker confirmed reduced drinking: Phosphatidyl ethanol, a biomarker that accumulates after alcohol consumption, dropped markedly in the semaglutide group and did not significantly change in placebo — corroborating the self-reported drinking reductions.
- Secondary metrics moved in the same direction: Lower total alcohol volume, fewer drinks per drinking day, lower craving scores, and more frequent two-step reductions on the WHO risk drinking levels scale.
- Substantial weight loss alongside the alcohol effect: Semaglutide arm lost 11.2 kg on average vs 2.2 kg on placebo; waist size and blood pressure also improved.
Source: The Lancet (2026) | Klausen, Fink-Jensen et al.
Alcohol use disorder accounts for roughly 5% of deaths worldwide each year and is a major driver of liver disease, cardiovascular disease, and several cancers.
The US Food and Drug Administration has approved only three medications for it — disulfiram, acamprosate, and naltrexone — and these are not universally effective and remain underutilized.
This trial tested whether semaglutide, a GLP-1 receptor agonist already approved for diabetes and obesity, could fill part of that treatment gap in patients with both alcohol use disorder and comorbid obesity.
108 Adults With Alcohol Use Disorder and Obesity Randomized to Semaglutide or Placebo
The trial was led by Mette Kruse Klausen and Anders Fink-Jensen at Copenhagen University Hospital, with collaborators at the US National Institutes of Health.
The design:
- Population: 108 adults split nearly evenly between men and women.
- Inclusion: Moderate-to-severe alcohol use disorder plus body mass index of 30+ (clinical obesity).
- Random assignment: 54 received once-weekly 2.4 mg semaglutide; 54 received weekly placebo (saline).
- Duration: 26 weeks.
- Setting: Single Danish clinical center.
- Adjunct therapy: All participants received up to 10 sessions of cognitive behavioral therapy focused on motivation, craving management, and relapse prevention.
To preserve blinding, participants wore blindfolds and listened to music through headphones during weekly injections, since the semaglutide pen makes a distinctive mechanical click.
Heavy Drinking Days Dropped 41.1 Points on Semaglutide vs 26.4 on Placebo
A heavy drinking day was defined as consuming at least 60 grams of pure alcohol for men or 48 grams for women.
The primary endpoint result:
- Semaglutide arm: 41.1 percentage point reduction in heavy drinking days over 26 weeks.
- Placebo arm: 26.4 percentage point reduction.
- Estimated treatment difference: 13.7 percentage points.
The placebo group’s substantial reduction reflects the cognitive behavioral therapy that all participants received plus the well-documented placebo response in alcohol use disorder trials. The semaglutide effect sits on top of that baseline.
An Objective Blood Biomarker Confirmed the Self-Reported Drop
Self-reported alcohol intake is a known weakness of addiction trials — participants under-report.
The Klausen team used phosphatidyl ethanol, a metabolite that accumulates in red blood cells after alcohol exposure, as an independent biological check.
The biomarker findings:
- Semaglutide arm: Phosphatidyl ethanol levels dropped markedly across the 26 weeks.
- Placebo arm: No statistically significant change.
The directional alignment between the biomarker and the self-reported heavy drinking days strengthens the efficacy claim. The drinking really did fall in the semaglutide arm, not just the reporting.
The Number Needed to Treat Was Lower Than the Approved Drugs
Number needed to treat (NNT) is the count of patients who must receive a medication for one to achieve a strong positive outcome — lower numbers mean a more effective drug.
The Klausen team reported an NNT of 4.3 for semaglutide in this trial.
For comparison, the FDA-approved alcohol use disorder medications (disulfiram, acamprosate, naltrexone) generally have an NNT of 7 or higher. The semaglutide signal is therefore notable, while still leaving open whether GLP-1 drugs can work broadly across addiction medicine.
Side-Effect Profile Was Mostly Gastrointestinal and Mostly Tolerable
Adverse effects clustered in the digestive system, consistent with semaglutide’s profile in obesity and diabetes use:
- Most common: Nausea, loss of appetite, vomiting, stomach pain.
- Severity: Mostly mild to moderate; tended to resolve within weeks.
- Liver enzymes: An enzyme linked to liver damage decreased sharply in the semaglutide arm — a favorable liver finding given that heavy alcohol use damages the liver.
- Pancreatic enzyme finding: Amylase rose slightly in some semaglutide patients but did not produce symptoms or serious pancreatic complications.
- Discontinuation: Only 4 participants left the semaglutide arm specifically due to side effects.
- Overall completion: 81% of enrolled participants completed the full 26-week intervention.
The tolerability is the practical hinge of the result. Drugs that work but cause unmanageable side effects do not close treatment gaps; this one appears to be tolerated well enough at the alcohol-use-disorder dose.
The Effect Did Not Generalize to Cigarette Smoking
One of the more useful negative findings is what the drug did not change.
Some participants were daily cigarette smokers at the start of the trial. Despite the substantial drop in alcohol consumption, these participants did not reduce tobacco use.
The cross-substance specificity carries a mechanistic implication. If the drug worked through a global “less reward seeking” effect, smoking should have moved with drinking.
It did not, suggesting the GLP-1 pathway acts more selectively on the alcohol reward circuit than on a general appetite-or-substance suppression mechanism.
Single-Site, Obesity-Restricted Sample, and Post-Treatment Follow-Up Stayed Out of Reach
- Single-center, small sample: 108 participants at one Danish clinic. The result needs replication in larger, multi-site, more demographically varied populations before broad clinical adoption.
- Obesity-restricted: Inclusion required BMI 30+, so the result cannot be extrapolated to alcohol use disorder patients without comorbid obesity. Whether semaglutide works for the broader AUD population remains unknown.
- Predominantly white sample: Limits generalization to other ancestry and demographic groups.
- CBT for everyone: All participants received cognitive behavioral therapy. The drug effect on top of CBT is what was measured; whether it would perform similarly without intensive psychological support is open.
- No post-treatment follow-up: The trial ended at 26 weeks. Whether reductions persist after discontinuation is unknown, and Matt Field at Sheffield flagged a likely rebound effect by analogy with appetite rebound after stopping semaglutide for weight loss.
A New Pharmacological Lever for Alcohol Use Disorder, Pending Replication
The clinical implications follow from the head-to-head comparison with existing options:
- Lower NNT than approved options: If the 4.3 NNT replicates, semaglutide would be the most effective single agent in the AUD pharmacological toolkit by that metric.
- Dual benefit population: Patients with both AUD and obesity get two clinical wins from a single weekly injection — the obesity comorbidity is clinically meaningful in a population already at high cardiometabolic risk.
- Reward-pathway target validates a broader strategy: The mechanistic story (GLP-1 receptors interacting with brain reward circuits) supports continued investigation of GLP-1 agents in other substance use disorders, while the negative cigarette finding cautions against generalizing prematurely.
- Open practical question on durability: The post-treatment rebound risk is the largest unknown. Future trials need extended follow-up to know whether semaglutide is a 26-week intervention or a longer-term maintenance therapy.
Citation: DOI: 10.1016/s0140-6736(26)00305-3. Klausen et al. Once-weekly semaglutide versus placebo in patients with alcohol use disorder and comorbid obesity: a randomised, double-blind, placebo-controlled trial. The Lancet. 2026.
Study Design: Randomized, double-blind, placebo-controlled trial at a single Danish clinical center; 26-week intervention; weekly subcutaneous injection plus up to 10 cognitive behavioral therapy sessions for all participants.
Sample Size: 108 adults with moderate-to-severe alcohol use disorder and BMI 30+; 54 randomized to 2.4 mg weekly semaglutide, 54 to placebo.
Key Statistic: Heavy drinking days reduced by 41.1 percentage points (semaglutide) vs 26.4 (placebo); estimated treatment difference 13.7 points; number needed to treat 4.3; phosphatidyl ethanol biomarker dropped markedly in semaglutide arm; weight loss 11.2 kg (semaglutide) vs 2.2 kg (placebo).
Caveat: Single-center, small sample, predominantly white, obesity-restricted; CBT for all participants may inflate apparent drug effect; no post-treatment follow-up so durability after discontinuation is unknown; semaglutide did not reduce cigarette smoking, suggesting cross-substance generalization is not automatic.