TL;DR: A 2026 study in The Pharmacogenomics Journal tested pharmacogenomic (PGx) depression care, meaning medication guidance based on drug-gene interactions; targeting Veterans already taking antidepressants with common PGx interactions raised the actionable-result rate to 30%, but immediate test-result access did not improve Patient Health Questionnaire-9 (PHQ-9) depression scores over 12 weeks.
Key Findings
- 60 Veterans were randomized: Researchers assigned 28 participants to immediate PGx results and 32 to delayed results after the 12-week trial.
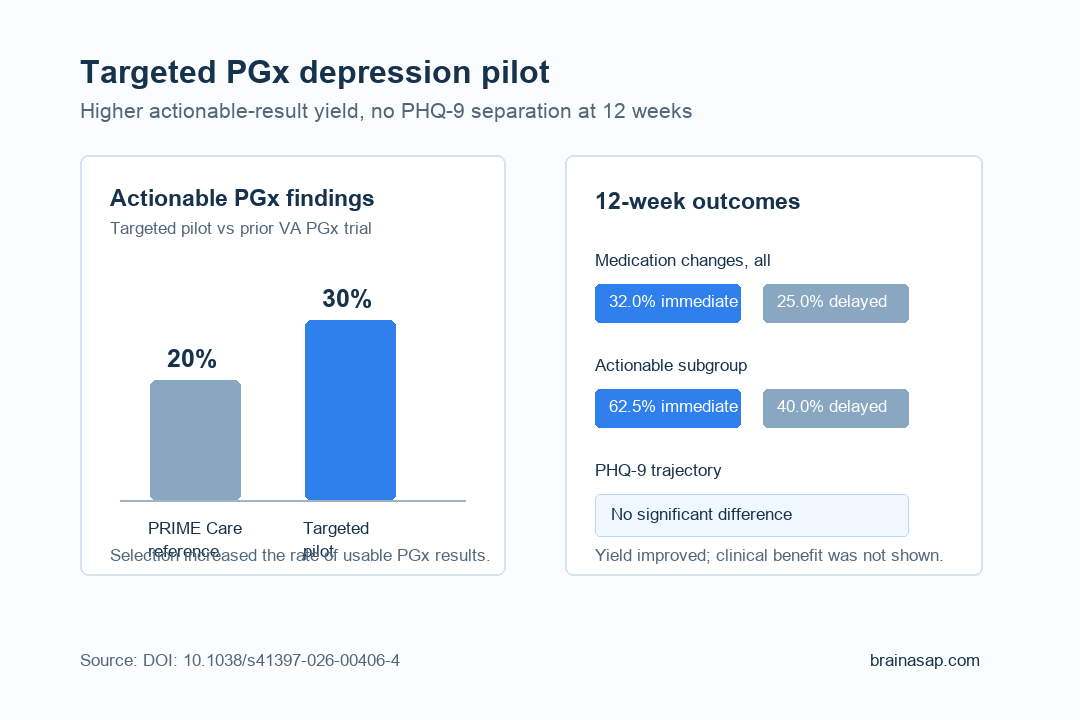
- Targeting changed the yield: The trial found 18 of 60 participants had an actionable drug-gene interaction, a 30% rate versus the 20% rate reported in the larger PRIME Care Veteran trial.
- Medication changes stayed statistically uncertain: Among actionable-genotype participants, medication changes occurred in 62.5% of the immediate-results group and 40.0% of the delayed-results group, but the confidence interval was wide.
- Depression scores did not separate: Repeated PHQ-9 analyses found no significant group-by-time difference across months 1, 2, and 3.
- Implementation mattered: Study authors argued that inconsistent clinician use of PGx reports likely weakened any real-world effect.
Source: The Pharmacogenomics Journal (2026) | Kennedy et al.
Why Targeted PGx Testing Was the Real Question
Pharmacogenomic testing in depression has a practical problem: many patients get a test result that does not actually change medication choice.
If most people in a trial do not have an actionable drug-gene interaction, even an effective PGx strategy can look weak because the test has little to act on.
Researchers tried to sharpen that problem. Instead of testing any patient with depression, they recruited Veterans who were already taking at least one antidepressant included on the Sanford Pharmacogenomics Panel.
The idea was straightforward: if the medication list is more likely to contain drugs affected by CYP2C19, CYP2D6, or related pharmacokinetic genes, the trial should find more cases where a PGx report could reasonably guide care.
The trial was about selection strategy as much as clinical benefit.
Researchers were not asking whether PGx testing should be handed out broadly to everyone with depression. They were asking whether a more targeted approach could identify a higher-yield group and make future trials more efficient.
How the 12-Week Veteran Trial Was Set Up
The study was a rater-blinded pragmatic randomized trial at the Corporal Michael J. Crescenz VA Medical Center.
Participants were Veterans aged 18 to 80 with a baseline PHQ-9 score above 9, an active depression diagnosis, and current antidepressant treatment that appeared on the Sanford PGx panel.
Researchers also required psychiatric polypharmacy, though the discussion later questions whether that criterion helped.
After blood draw, participants were randomized into 2 arms:
- Immediate-results arm: Clinicians received the PGx report within about a week and could use it during ordinary care.
- Delayed-results arm: Clinicians received the report only after the 12-week study window ended.
- Blinded rating: PHQ-9 depression scores were assessed monthly by raters who were blinded to clinical status and treatment assignment.
The design mirrored real clinic friction. The PGx report did not force a medication change.
It gave clinicians information, and then the trial measured whether that information changed prescribing behavior, timing, or depression symptoms.
Actionable Results Rose, but Symptom Benefit Did Not
The strongest positive finding was the enrichment signal. Overall, 18 of 60 Veterans had an actionable gene-drug interaction, including 8 of 28 in the immediate-results arm and 10 of 32 in the delayed-results arm.
The actionable variants were mainly CYP2C19 rapid-metabolizer findings tied to medications such as sertraline and escitalopram.
The medication-change pattern pointed in the expected direction but was too small to settle the question. Among participants with actionable genotypes, 5 of 8 in the immediate-results arm and 4 of 10 in the delayed-results arm had a medication change.
The estimated odds ratio was 2.50, but the 95% confidence interval ran from 0.37 to 16.89, which means the study could not distinguish a real effect from noise.
Across all participants, the difference was also modest: 32.0% of the immediate arm and 25.0% of the delayed arm had a medication change. Time to first medication change did not improve either.
Median time was 66 days in the immediate arm versus 59.5 days in the delayed arm.
The depression-score result was the clearest negative finding. PHQ-9 trajectories did not significantly differ by group.
This small pragmatic trial did not show a 12-week symptom advantage from giving clinicians the report immediately.
The Clinician-Use Problem May Be the Main Signal
The study’s most important lesson may be about implementation. A PGx report can only help if clinicians see it, understand it, trust it, and act when the recommendation fits the patient.
In this trial, researchers explicitly noted poor application of PGx results by clinicians, which would reduce study power and clinical value.
That is an important distinction. A failed medication-change pathway can come from several places:
- No actionable result: The patient has no relevant drug-gene interaction on the panel.
- Actionable result, no clinical fit: The report suggests a change, but symptoms, side effects, prior response, or patient preference argue against switching.
- Actionable result, no implementation: The report could guide care, but it does not reach the appointment or clinician workflow in time.
- Actionable result, unclear outcome window: A medication change happens, but 3 months may be too short or too noisy to detect a symptom difference.
This pilot points especially toward the third problem. PGx testing may require pharmacists, decision support, scheduling alignment, or clinician education to convert a genetic result into an appropriate prescribing decision.
Without that workflow, the test becomes information sitting beside the clinical process rather than inside it.
What a Larger Depression PGx Trial Would Need
The power calculation in the discussion puts the result in practical terms. Based on the observed medication-change difference among actionable-genotype patients, researchers estimated that a future trial would need 160 participants with actionable genotypes to have 80% power.
With the study’s 30% actionable-result rate, that would mean about 533 tested participants. With a 20% actionable-result rate, it would mean about 800.
The enrichment strategy remains important even without a positive PHQ-9 result. If future trials can start with patients more likely to have drug-gene interactions, they can test PGx-guided depression care with fewer randomized participants and a clearer clinical target.
The next version also needs tighter care delivery. Study authors suggested clinician education, pharmacist interpretation, better timing around appointments, and possibly pharmacist-led recommendations.
Those are not side details. In real depression care, they may determine whether PGx testing is a clinically relevant prescribing tool or just another lab result with weak follow-through.
Citation: DOI: 10.1038/s41397-026-00406-4. Study authors et al. Kennedy et al. A pilot study of pharmacogenomic testing as a tool to enhance depression care in Veterans. The Pharmacogenomics Journal . 2026;26:14.
Study Design: Rater-blinded 12-week pragmatic randomized clinical pilot trial.
Sample Size: 60 Veterans with depression receiving antidepressant treatment; 28 immediate-results and 32 delayed-results participants.
Key Statistic: 30% had an actionable PGx drug-gene interaction; PHQ-9 group-by-time effects were not significant.
Caveat: The trial was underpowered and clinician use of PGx reports was inconsistent.