TL;DR: A 2026 secondary analysis in PLOS One found that low-intensity focused ultrasound and repetitive transcranial magnetic stimulation (rTMS) had similar short-term post-stroke motor endpoint scores, while change-from-baseline Fugl-Meyer gains were larger with focused ultrasound.
Key Findings
- 50-person comparison: The analysis compared 25 subacute stroke patients assigned to LIFU with 25 assigned to rTMS.
- 10 sessions: Both neuromodulation groups received 20-minute sessions 5 days per week for 2 weeks, plus standard rehabilitation.
- Endpoints did not separate: Post-intervention FMA, Modified Barthel Index, and Brunnstrom stage comparisons showed no significant between-group differences.
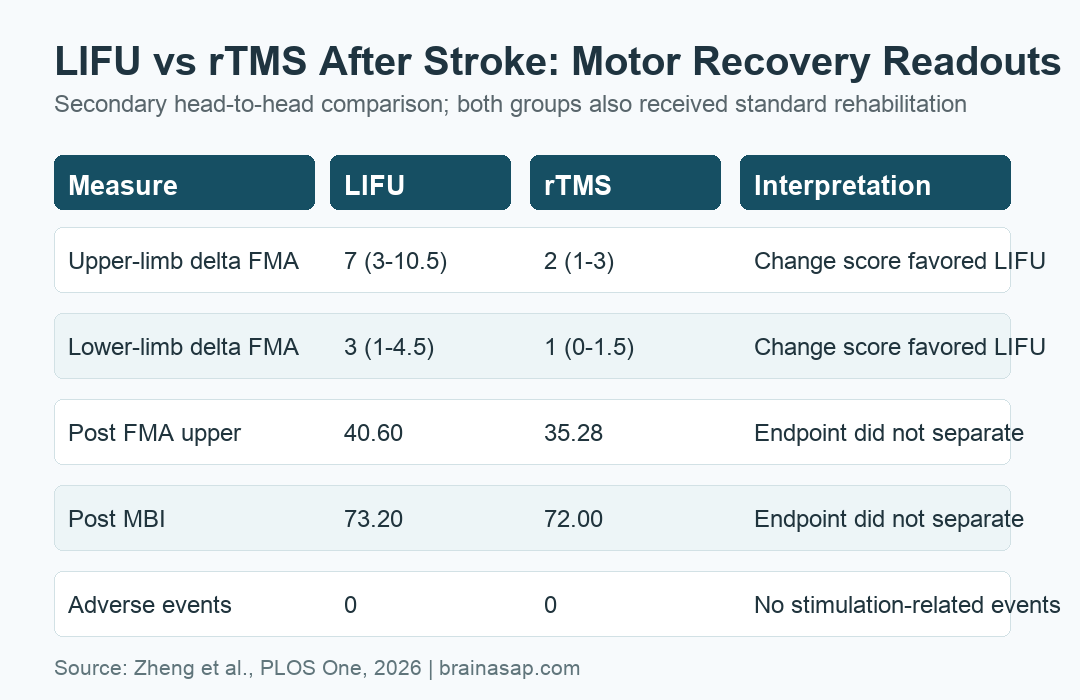
- Change scores favored LIFU: Median upper-limb delta FMA was 7 with LIFU versus 2 with rTMS; lower-limb delta FMA was 3 versus 1.
- No stimulation events: No stimulation-related adverse events were observed in either neuromodulation group.
Source: PLOS One (2026) | Zheng et al.
Low-intensity focused ultrasound (LIFU) and repetitive transcranial magnetic stimulation (rTMS) are both non-invasive neuromodulation approaches being studied as rehabilitation add-ons after stroke. The analysis compared the 2 stimulation arms directly.
The clinical results split by outcome type. Both groups improved over 2 weeks, endpoint scores were statistically similar, and LIFU showed larger change-from-baseline Fugl-Meyer Assessment gains.
LIFU and rTMS Targeted the Ipsilesional Motor Cortex
The source trial randomized 75 people into 3 arms: standard rehabilitation alone, rehabilitation plus LIFU, or rehabilitation plus rTMS. The secondary analysis used only the 2 active neuromodulation arms, leaving 50 participants in the head-to-head comparison.
Participants had subacute stroke, unilateral limb motor dysfunction, and stable neurological status before enrollment. The stimulation target was the ipsilesional primary motor cortex, meaning the motor-cortex region on the side of the brain affected by the stroke.
- LIFU protocol: 0.5 MHz ultrasound, 20-minute sessions, 5 days per week for 2 weeks.
- rTMS protocol: 10 Hz stimulation at 80% resting motor threshold, 1,000 pulses per session.
- Rehabilitation base: All participants received physical and occupational therapy during the 2-week period.
- Blinding: Outcome assessors and data analysts were blinded, but participants and therapists were not.
Both Groups Improved on Motor and Daily-Function Measures
The main clinical scale was the Fugl-Meyer Assessment (FMA), a standardized stroke motor-impairment measure. In the LIFU group, upper-limb FMA improved from 32.00 to 40.60, and lower-limb FMA improved from 22.68 to 26.60.
The rTMS group also improved. Upper-limb FMA moved from 32.20 to 35.28, and lower-limb FMA moved from 23.96 to 25.24.
- LIFU within-group gains: Upper- and lower-limb FMA and Modified Barthel Index scores improved with p values below 0.001.
- rTMS within-group gains: FMA and Modified Barthel Index scores also improved significantly.
- Brunnstrom stages: Motor recovery stages improved in both groups.
Those within-group changes are encouraging, but they do not by themselves prove one stimulation method is better. Stroke recovery during the subacute period can be driven by standard rehabilitation and spontaneous biological recovery.
Post-Treatment Endpoint Scores Did Not Show a Clear Winner
The primary between-group endpoint comparisons were based on post-intervention scores. On those comparisons, LIFU and rTMS did not significantly differ for upper-limb FMA, lower-limb FMA, Modified Barthel Index, or Brunnstrom stages.
For example, post-treatment upper-limb FMA was 40.60 with LIFU and 35.28 with rTMS, but the unadjusted endpoint comparison was not significant. Post-treatment Modified Barthel Index scores were 73.20 and 72.00.
- Upper-limb endpoint: No significant post-treatment group difference in the primary unadjusted comparison.
- Lower-limb endpoint: No significant post-treatment group difference.
- Daily function: Modified Barthel Index endpoint scores were similar.
- Clinical interpretation: The endpoint results do not establish superior short-term efficacy for either modality.
Change-From-Baseline FMA Gains Were Larger With LIFU
The more favorable LIFU signal came from change scores. Median upper-limb delta FMA was 7 in the LIFU group versus 2 in the rTMS group, with p = 0.001.
Lower-limb delta FMA showed the same direction: 3 with LIFU versus 1 with rTMS, with p below 0.001. These change-score findings suggest different recovery dynamics during the 2-week intervention period.
- Helpful signal: LIFU had larger median motor-change scores.
- Endpoint boundary: Those gains did not translate into significant unadjusted post-treatment endpoint separation.
- Power boundary: The secondary comparison had about 78% power for a medium effect size, slightly below the conventional 80% threshold.
These data support larger head-to-head LIFU trials, but they do not prove clinical superiority over rTMS.
fNIRS Suggested Different Cortical Activity Patterns
The analysis also used functional near-infrared spectroscopy (fNIRS), a non-invasive optical method for tracking cortical blood-oxygenation signals. These neuroimaging outcomes were exploratory.
Prefrontal fractional amplitude of low-frequency fluctuations (fALFF), an index of spontaneous cortical activity, increased in the LIFU group with p = 0.002. The rTMS group did not show a significant prefrontal fALFF change.
- Between-group fALFF change: Motor-related delta fALFF was 0.028 with LIFU versus -0.018 with rTMS.
- Connectivity caution: Functional connectivity changes did not remain significant after correction for multiple comparisons.
- Mechanism boundary: Resting-state fNIRS does not prove the neural mechanism behind motor recovery.
The imaging data are useful for hypothesis generation. They suggest LIFU and rTMS may modulate cortical networks differently, but they do not replace the clinical endpoint results.
Small Secondary Design Limits the Head-to-Head Claim
No stimulation-related adverse events were observed in either group, and all participants tolerated the neuromodulation course without serious neurological complications or treatment interruptions.
The limitations are substantial: this was a secondary head-to-head comparison, not an independently powered direct superiority trial. The intervention lasted only 2 weeks, follow-up was immediate, and lesion-specific or stroke-phase subgroups were not analyzed.
For rehabilitation research, LIFU appeared feasible and produced larger change scores. The next test needs a larger prospective trial with longer follow-up and prespecified LIFU-versus-rTMS power.
Citation: DOI: 10.1371/journal.pone.0348030. Zheng et al. A secondary head-to-head comparison of low-intensity focused ultrasound and repetitive transcranial magnetic stimulation for motor recovery after stroke. PLOS One. 2026;21(4):e0348030.
Study Design: Secondary head-to-head analysis from a prospectively registered randomized controlled trial.
Sample Size: 50 subacute stroke patients in the LIFU and rTMS arms, with 43 completing all intervention sessions and assessments.
Key Statistic: Median upper-limb delta FMA was 7 with LIFU versus 2 with rTMS, while post-treatment endpoint scores did not significantly differ.
Caveat: The comparison was secondary, modestly powered, short-term, and not sufficient to prove LIFU superiority over rTMS.