TL;DR: A 2026 methodology paper in European Archives of Psychiatry and Clinical Neuroscience describes EMBER-MDD, a research-only multi-omic study designed to find treatment-resistance and esketamine-response biomarkers in about 420 adults with major depressive disorder.
Key Findings
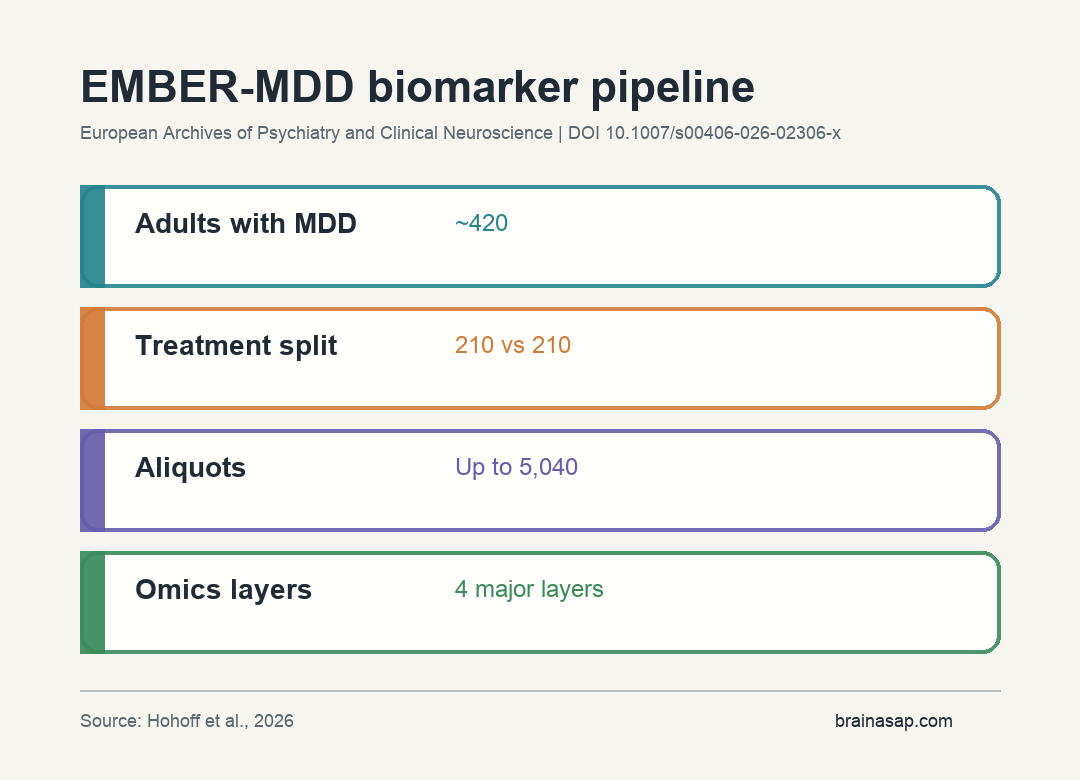
- About 420 adults: EMBER-MDD will analyze biomaterials from approximately 420 adults with major depressive disorder.
- 210 versus 210 design: The planned comparison estimates 210 esketamine-treated participants and 210 treatment-as-usual participants.
- Up to 5,040 aliquots: Whole blood, RNA-stabilized blood, plasma, and serum are stored at minus 80 degrees C across baseline and follow-up time points.
- Four omics layers: The study combines genomics, epigenomics, transcriptomics, and proteomics/metabolomics.
- Research-only output: The authors state that EMBER-MDD will not support individual efficacy, tolerability, or clinical decision-making.
Source: European Archives of Psychiatry and Clinical Neuroscience (2026) | Hohoff et al.
Esketamine biomarkers are a practical problem because treatment-resistant depression is often recognized late. Clinicians usually learn that a patient is resistant only after multiple treatment attempts have already failed.
EMBER-MDD is not a new efficacy trial. It is a non-interventional, investigator-initiated in-vitro study that will analyze stored biospecimens from INTENSIFY and OBS-TR participants after treatment is complete.
That distinction should stay visible. The paper is about how to build a molecular evidence base around treatment resistance and esketamine response, not about proving that esketamine works better for an individual patient in the clinic today.
EMBER-MDD Targets Treatment-Resistant Depression Earlier
Treatment resistance affects roughly one-third of patients with major depressive disorder, according to the paper’s background framing. That creates a delay: intensified care may arrive only after a patient has already spent months or years cycling through standard options.
The broader Psych-STRATA program is designed to identify molecular signatures of treatment resistance across severe psychiatric illnesses. EMBER-MDD is the major-depression biomarker arm focused on esketamine nasal spray versus treatment as usual.
This makes the study partly a depression project and partly an infrastructure project. It links trial-era clinical information to frozen biospecimens so that molecular data can be interpreted against actual treatment paths.
The study asks 2 related questions:
- Risk question: Which molecular patterns are associated with treatment-resistance risk?
- Response question: Which molecular patterns correlate with clinical response to esketamine compared with usual treatment?
Blood-Based Biospecimens Will Feed Four Omics Layers
The planned biomaterial set is large for a psychiatric biomarker study. Researchers expect samples from approximately 420 adults with MDD, split into an estimated 210 esketamine and 210 treatment-as-usual participants.
The split is important because a response biomarker has to distinguish more than illness severity. It needs to tell researchers whether a molecular pattern is associated with esketamine response, usual-care response, or treatment resistance across both groups.
The sample types include whole blood, RNA-stabilized whole blood, plasma, and serum. Collection occurs at baseline and, when feasible, during and after treatment, generating up to 5,040 stored aliquots.
EMBER-MDD will analyze several molecular layers:
- Genomics: Baseline DNA genotyping on Illumina Infinium GSA v3.0+MD arrays.
- Epigenomics: Genome-wide DNA methylation profiling across time points with MethylationEPIC v2.0.
- Transcriptomics: mRNA sequencing using NovaSeq X or X Plus platforms.
- Proteomics and metabolomics: High-throughput Olink and/or Biocrates platforms.
Machine Learning Is Planned After Individual Omics Analysis
The paper lays out a layered analysis plan. Each omics layer will first undergo its own preprocessing and analysis, including approaches such as genome-wide association, polygenic-risk scoring, epigenome-wide association, differential expression, pathway analysis, and network analysis.
The integrative step is the higher-risk, higher-value part. EMBER-MDD plans QTL mapping across molecular layers and intermediate-fusion machine learning with nested cross-validation.
The analysis plan also names explainable-AI methods, including SHAP and LIME, to connect prediction back to interpretable features. Black-box biomarker models are hard to trust in psychiatry unless they point to biology that can be tested again.
Nested cross-validation is another quality-control piece. It is meant to reduce the risk that a model looks accurate because it learned quirks of one dataset rather than a reproducible treatment-resistance signal.
The Study Is Explicitly Research-Only
The strongest guardrail in the paper is also the easiest one to miss. EMBER-MDD outputs are described as research-only. They will not support individual efficacy, tolerability, or clinical decision-making.
Biomarker language can sound more clinically ready than it is. A signature discovered in stored samples still needs independent validation, prospective testing, and evidence that it changes outcomes before it can guide care.
The paper’s near-term value is therefore not a test a patient can order. It is a structured attempt to identify candidate biosignatures and mechanisms that future trials can validate.
If the approach works, the next step would be prospective validation: measure the candidate biomarkers before treatment, assign or predict treatment paths, and test whether the biomarker improves outcomes compared with ordinary clinical judgment.
Missing Data and Generalizability Are Built-In Risks
Multi-omic psychiatry studies are vulnerable to missingness. Some patients may not provide complete data across all sample types, molecular layers, and time points.
If more severely ill or less adherent patients are underrepresented in some layers, the model can become biased.
The paper names imputation, sensitivity analyses, and robust feature selection as mitigation strategies. Those methods can reduce bias, but they cannot fully remove it.
Generalizability is another limit. The sample comes from specific clinical services and treatment protocols.
A biomarker pattern from esketamine versus second-line antidepressant care may not transfer cleanly to psychotherapy-focused pathways, neuromodulation, older populations, or different health systems.
Citation: DOI: 10.1007/s00406-026-02306-x. Hohoff et al. Esketamine multi-omic biomarker evaluation in major depressive disorder (EMBER-MDD): concept, objectives and methodologies of a non-clinical investigator-initiated study. European Archives of Psychiatry and Clinical Neuroscience. 2026.
Study Design: Non-interventional, investigator-initiated in-vitro multi-omic biomarker study using post-treatment biospecimens from INTENSIFY and OBS-TR.
Sample Size: Approximately 420 adults with major depressive disorder, with an estimated 210 esketamine and 210 treatment-as-usual participants.
Key Statistic: Up to 5,040 biospecimen aliquots will support genomics, epigenomics, transcriptomics, and proteomics/metabolomics analyses.
Caveat: Results are research-only and cannot guide individual esketamine prescribing without prospective validation.