TL;DR: A 2026 review in Translational Psychiatry argues for a biologically meaningful inflammatory depression subgroup, with CRP, IL-6, TNF-alpha, glial activation, kynurenine metabolism, and synaptic plasticity linking immune signaling to symptoms and treatment response.
Key Findings
- One-third treatment gap: The review notes that current pharmacological treatments fail to produce adequate responses in approximately one-third of patients with major depressive disorder.
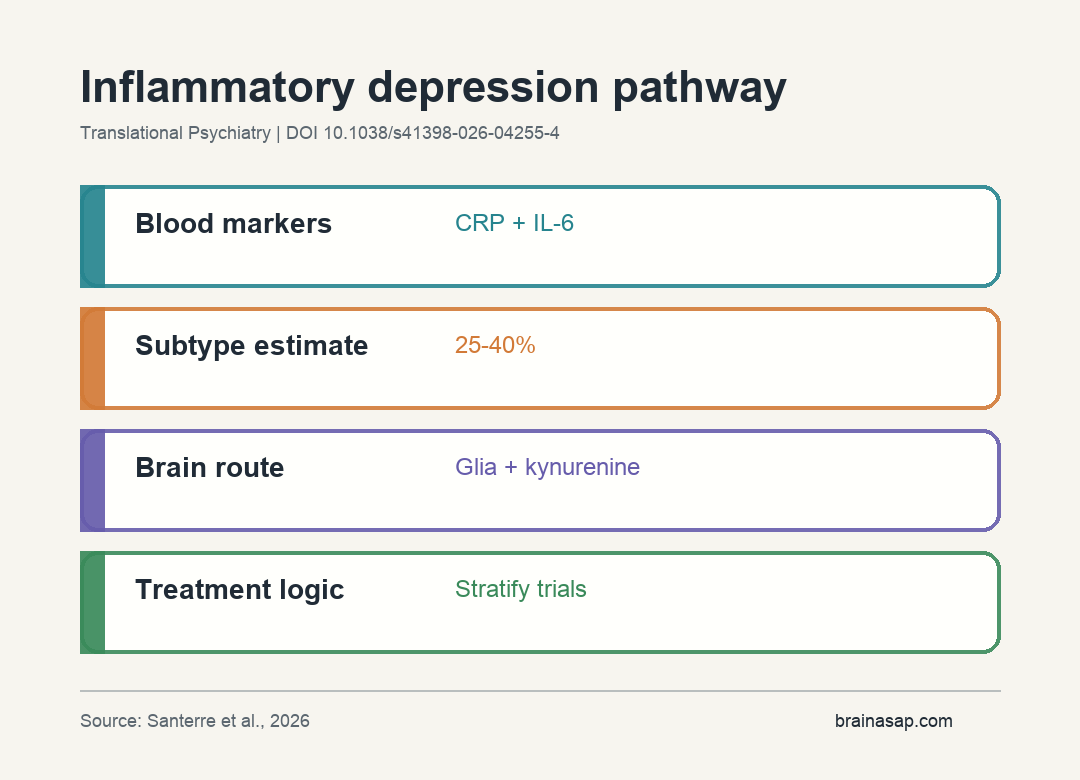
- 25-40% inflammatory subgroup: The authors describe an inflammatory depression subtype estimated at 25% to 40% of clinical samples using CRP thresholds above 3 mg/L.
- Core blood markers: C-reactive protein, interleukin-6, tumor necrosis factor-alpha, and interleukin-1beta are repeatedly elevated in depression meta-analyses.
- Multiple brain routes: Immune signaling is linked to IDO1-driven serotonin depletion, AMPA receptor internalization, HPA-immune feedback dysregulation, and reduced plasticity.
- Stratified-treatment claim: Elevated inflammatory markers are positioned as signals for patients less likely to respond to conventional antidepressants and more likely to need anti-inflammatory strategies.
Source: Translational Psychiatry (2026) | Santerre et al.
Neuroinflammation in depression is not a claim that all depression is inflammation. Santerre’s team reviews immune-brain pathways involved in symptoms and treatment response in a sizable patient subgroup.
The synthesis spans blood biomarkers, post-mortem work, positron emission tomography, transcriptomics, and treatment studies. Its clinical argument is stratification: depression needs immune-informed subtyping rather than one biological explanation.
Inflammatory Depression Is Framed as a Subtype, Not the Whole Disease
The review estimates that 25% to 40% of clinical depression samples show an inflammatory subtype when CRP thresholds above 3 mg/L are used. That is a large minority, not a universal rule.
This framing avoids a common mistake. Depression is clinically heterogeneous, and no single pathway explains every case.
Inflammatory biology is central for some patients, secondary for others, and irrelevant for another group.
That subgroup framing shifts the question from whether inflammation causes depression in general to which patients have enough inflammatory activity for immune biology to shape symptoms and treatment response.
The authors connect inflammatory depression to a recognizable clinical pattern:
- Immune markers: Higher CRP, IL-6, TNF-alpha, and IL-1beta in blood-based studies.
- Treatment resistance: Poorer response to conventional antidepressants when inflammatory tone is elevated.
- Candidate response path: Greater potential relevance for anti-inflammatory or immune-modulating strategies.
CRP and IL-6 Are More Consistent Than Short-Lived Cytokines
The review highlights C-reactive protein, interleukin-6, tumor necrosis factor-alpha, and interleukin-1beta as repeatedly elevated markers in depression meta-analyses. It also cautions that cytokine measurement is technically uneven.
CRP and IL-6 are generally more consistent than lower-concentration or shorter-lived cytokines such as IL-1beta and TNF-alpha. Pre-analytical handling, protein stability, and assay sensitivity can change what a study detects.
For a future clinic-facing tool, that reliability difference affects feasibility. A cheap and stable marker is often less biologically specific than a cytokine panel, but it can be more practical if it is measured consistently across settings.
Biomarker stratification only works if the marker is reliable enough for the job. A noisy cytokine panel can create false precision.
That is why the review treats marker choice as a clinical-design problem, not a simple lab preference.
Immune Signaling Can Reach Mood Biology Through Several Routes
The review does not reduce depression to a single inflammatory molecule. It describes several routes by which immune activation can influence neural systems involved in mood and motivation.
Key pathways include:
- IDO1 and tryptophan: Inflammatory signaling can shift tryptophan metabolism away from serotonin-relevant pathways and toward kynurenine products.
- Glutamate signaling: Cytokine-mediated AMPA receptor internalization is described as altering excitatory transmission.
- HPA-immune feedback: Stress-hormone and immune circuits can reinforce each other when regulation breaks down.
- Plasticity loss: Glial activation and inflammatory signaling are described as suppressing BDNF-related synaptic maintenance.
These mechanisms connect immune markers to depression-relevant neurobiology rather than treating inflammation as a vague background state.
They also explain why inflammatory depression often looks motivational and cognitive, not only sad. Changes in tryptophan metabolism, glutamatergic signaling, and synaptic plasticity plausibly affect fatigue, reward processing, concentration, and psychomotor slowing.
Subgroup trials should measure those domains alongside mood symptoms.
Brain Evidence Is Consistent but Still Not Definitive
The review cites post-mortem studies, TSPO-PET imaging of translocator protein density, and transcriptomic analyses as evidence linking microglial activation to depression neurobiology. The authors still treat the evidence as not fully definitive.
That caution is appropriate. TSPO-PET can be affected by genetics and ligand-binding issues, post-mortem tissue is shaped by illness and treatment history, and transcriptomic findings depend on tissue source and analytic choices.
The supported interpretation is specific: multiple methods point toward glial and immune involvement in depression, but the field still needs cleaner patient stratification and prospective tests.
Biomarker-Guided Treatment Is the Practical Goal
The review’s clinical direction is stratified treatment. If inflammatory depression is identified reliably, trials should test anti-inflammatory strategies in the patients most likely to benefit rather than diluting effects across all depression.
A failed anti-inflammatory trial in an unselected depression sample does not prove the pathway is irrelevant. It can mean the subgroup was too small or poorly measured.
For now, the clinical message is cautious. CRP, IL-6, and related markers help define an inflammatory subtype, but they are not standalone diagnostic tests for depression and should not replace symptom-based assessment or validated treatment algorithms.
The review therefore supports biomarker-enriched trials more strongly than immediate biomarker prescribing. The evidence is strong enough to justify better subgroup testing, but not strong enough to treat one blood marker as a complete treatment map.
Citation: DOI: 10.1038/s41398-026-04255-4. Santerre et al. Neuroinflammation and depression: immune-brain interface mechanisms, biomarker stratification, and therapeutic strategies. Translational Psychiatry. 2026.
Study Design: Narrative mechanistic review of neuroinflammatory pathways, blood biomarkers, brain evidence, and therapeutic-stratification strategies in depression.
Sample Size: Not a primary cohort; the review synthesizes evidence from population cohorts, clinical samples, experimental models, imaging, post-mortem, and transcriptomic studies.
Key Statistic: The review estimates an inflammatory depression subtype in 25% to 40% of clinical samples at CRP thresholds above 3 mg/L.
Caveat: Biomarker findings vary by assay, sample handling, patient selection, and whether peripheral markers reflect central inflammatory processes.