TL;DR: A 2026 real-world study in Journal of Clinical Sleep Medicine found that glucagon-like peptide-1 receptor agonist use was associated with lower 3-year cardiovascular-event risk in adults with obesity and obstructive sleep apnea.
Key Findings
- 18,523 matched pairs: Propensity matching compared GLP-1 receptor agonist users with similar non-users who had obesity and obstructive sleep apnea.
- 24% lower heart-failure hazard: New heart failure was less common in GLP-1RA users over 3 years (HR 0.76; 95% CI 0.71-0.82).
- 33% lower pulmonary hypertension hazard: Pulmonary hypertension was also lower in the treated cohort (HR 0.67; 95% CI 0.59-0.75).
- 43% lower all-cause mortality hazard: Death from any cause was lower among GLP-1RA users (HR 0.57; 95% CI 0.51-0.63).
- Observational evidence: The study can show association, not prove that GLP-1RAs caused the cardiovascular differences.
Source: Journal of Clinical Sleep Medicine (2026) | Ahn et al.
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are drugs used for diabetes and weight management, with cardiovascular benefits already reported in several high-risk groups. This study asked whether those benefits also appeared in people with obstructive sleep apnea (OSA) and obesity.
OSA, obesity, type 2 diabetes, hypertension, and cardiovascular disease often cluster in the same patients. In this matched cohort, GLP-1RA exposure tracked lower cardiovascular hazards in that overlapping clinical population.
GLP-1RAs Were Linked to Lower 3-Year Heart Failure in Obstructive Sleep Apnea
The analysis used TriNetX, a large real-world health-record network. Researchers identified adults with OSA and body mass index above 30 who did not already have heart failure, pulmonary hypertension, or myocardial infarction at baseline.
Patients were split into two groups: those prescribed a GLP-1RA within 1 year of OSA diagnosis and those never prescribed one. Before matching, the treated cohort included 18,774 people, while the comparison cohort included 847,137 people.
- Exposure group: GLP-1RA prescription within 1 year after OSA diagnosis.
- Comparison group: No GLP-1RA prescription in the health-record data.
- Follow-up window: Cardiovascular outcomes were tracked for 3 years.
After propensity-score matching, each group had 18,523 patients. The matched cohorts were similar on age, sex, race, body mass index, hemoglobin A1c, medication use, and major baseline comorbidities.
The primary result was new heart failure. GLP-1RA users had 1,416 cases of heart failure, compared with 1,791 cases among matched non-users, corresponding to a hazard ratio of 0.76.
Mortality, Pulmonary Hypertension, and Heart Attack Hazards Were Also Lower
The secondary outcomes moved mostly in the same direction. All-cause mortality showed the largest relative difference: 550 deaths in the GLP-1RA cohort versus 945 in the non-user cohort.
Acute myocardial infarction, or heart attack, was also lower. Researchers reported 417 cases among GLP-1RA users and 535 among non-users, with a hazard ratio of 0.76.
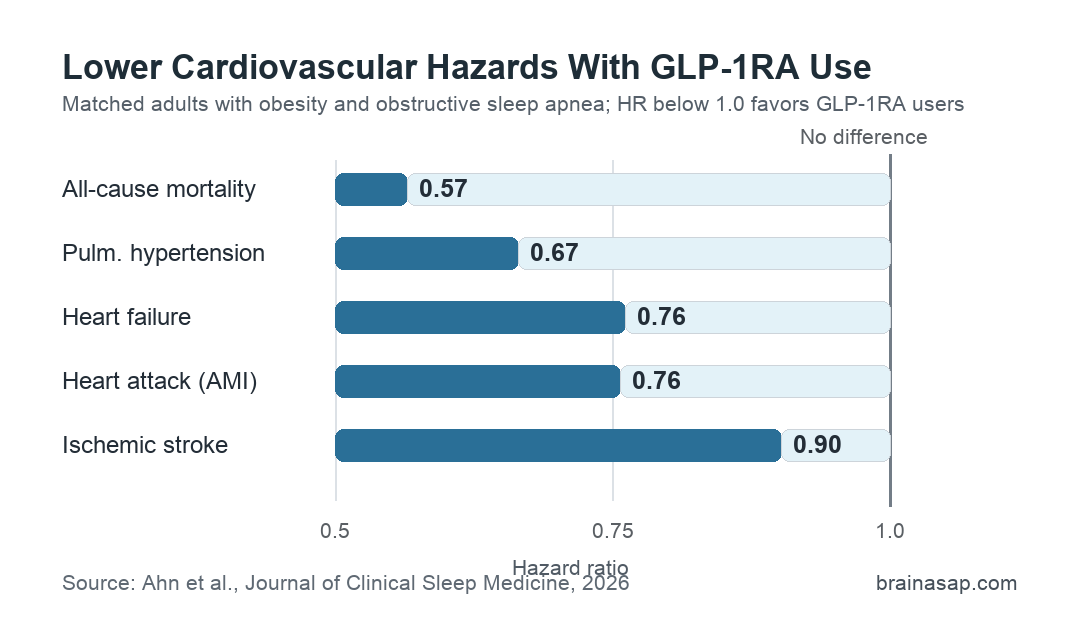
- All-cause mortality: HR 0.57, with a 95% confidence interval of 0.51 to 0.63.
- Pulmonary hypertension: HR 0.67, with a 95% confidence interval of 0.59 to 0.75.
- Acute myocardial infarction: HR 0.76, with a 95% confidence interval of 0.67 to 0.86.
- Ischemic stroke: HR 0.90, with a 95% confidence interval of 0.82 to 0.99.
Stroke was the weakest of the reported associations, with a hazard ratio close to 1.0. The other outcomes showed larger relative differences and narrower-looking separation in the reported survival curves.
The study also broke heart-failure risk down by drug class. Dulaglutide, semaglutide, and liraglutide each remained associated with lower heart-failure hazard, although this subgroup analysis should be read as exploratory.
Matched Cohorts Still Leave Room for Confounding by Treatment Selection
Propensity matching is useful because GLP-1RA users and non-users were very different before adjustment. For example, before matching, type 2 diabetes appeared in 82.1% of GLP-1RA users but only 21.7% of non-users.
After matching, type 2 diabetes was common in both groups, and body mass index was nearly identical. The comparison therefore relied on more similar baseline groups than the raw treated-versus-untreated contrast.
- Large scale: The final matched sample included more than 37,000 patients.
- Balanced baseline measures: Demographics, medications, body mass index, and HbA1c were closely aligned after matching.
- Outcome exclusions: Patients with prior heart failure, pulmonary hypertension, or myocardial infarction were excluded before follow-up.
Even so, matched observational data cannot eliminate every treatment-selection difference. GLP-1RA users may differ in health-care access, medication adherence, weight change, diabetes management, positive airway pressure use, or clinical monitoring in ways not fully captured by the database.
The paper also relied on diagnosis codes and prescription records. That means OSA severity, actual medication persistence, weight loss over time, and positive airway pressure adherence were not measured with the same detail as they would be in a purpose-built trial.
OSA Cardiovascular Risk May Need Both Airway and Metabolic Treatment
OSA is often discussed through the airway lens: breathing interruptions, oxygen drops, sleep fragmentation, and positive airway pressure therapy. This study supports a complementary view in which metabolic treatment may also matter for cardiovascular outcomes in patients with OSA and obesity.
The association fits prior evidence that GLP-1RAs can improve cardiometabolic risk, while tirzepatide trials have reported improvements in apnea-hypopnea index and inflammatory or blood-pressure measures. This study did not test tirzepatide as the central exposure, but it adds real-world evidence for selective GLP-1RA use in an OSA population.
- Clinical interpretation: The association is strongest as a risk-modifier signal, not proof of a new OSA indication.
- Patient context: The findings apply to patients with obesity and OSA, many of whom also had diabetes and hypertension.
- Next study need: Prospective trials should measure OSA severity, weight change, medication adherence, and airway-therapy adherence together.
The cohort supports a narrower statement than “GLP-1RAs treat sleep apnea.” GLP-1RA users with OSA and obesity had lower 3-year hazards for several cardiovascular outcomes than similar non-users.
Citation: DOI: 10.1007/s44470-026-00110-x. Ahn et al. Glucagon-like peptide receptor agonists (GLP-1RAs) as cardiovascular risk modifiers in obstructive sleep apnea and obesity: a real-world study. Journal of Clinical Sleep Medicine. 2026;22:102.
Study Design: Propensity-score matched retrospective cohort study using TriNetX real-world health-record data.
Sample Size: 18,523 GLP-1RA users and 18,523 matched non-users with obesity and obstructive sleep apnea.
Key Statistic: New heart failure was lower in GLP-1RA users over 3 years (HR 0.76; 95% CI 0.71-0.82).
Caveat: The study was observational and cannot prove that GLP-1RAs caused the lower cardiovascular risks.