TL;DR: A 2026 preprint posted on medRxiv reported that resting-state electroencephalography (EEG) neural slowing after stroke tracked secondary thalamic degeneration measured on structural MRI, even though the sampled patients did not have direct thalamic lesions.
Key Findings
- 25 stroke patients: Researchers studied adults at least 3 months after unilateral supratentorial stroke and compared their resting-state EEG data with 17 controls.
- No direct thalamus damage: Patients with thalamic lesions or vascular-territory evidence of primary thalamic injury were excluded, keeping the focus on secondary degeneration.
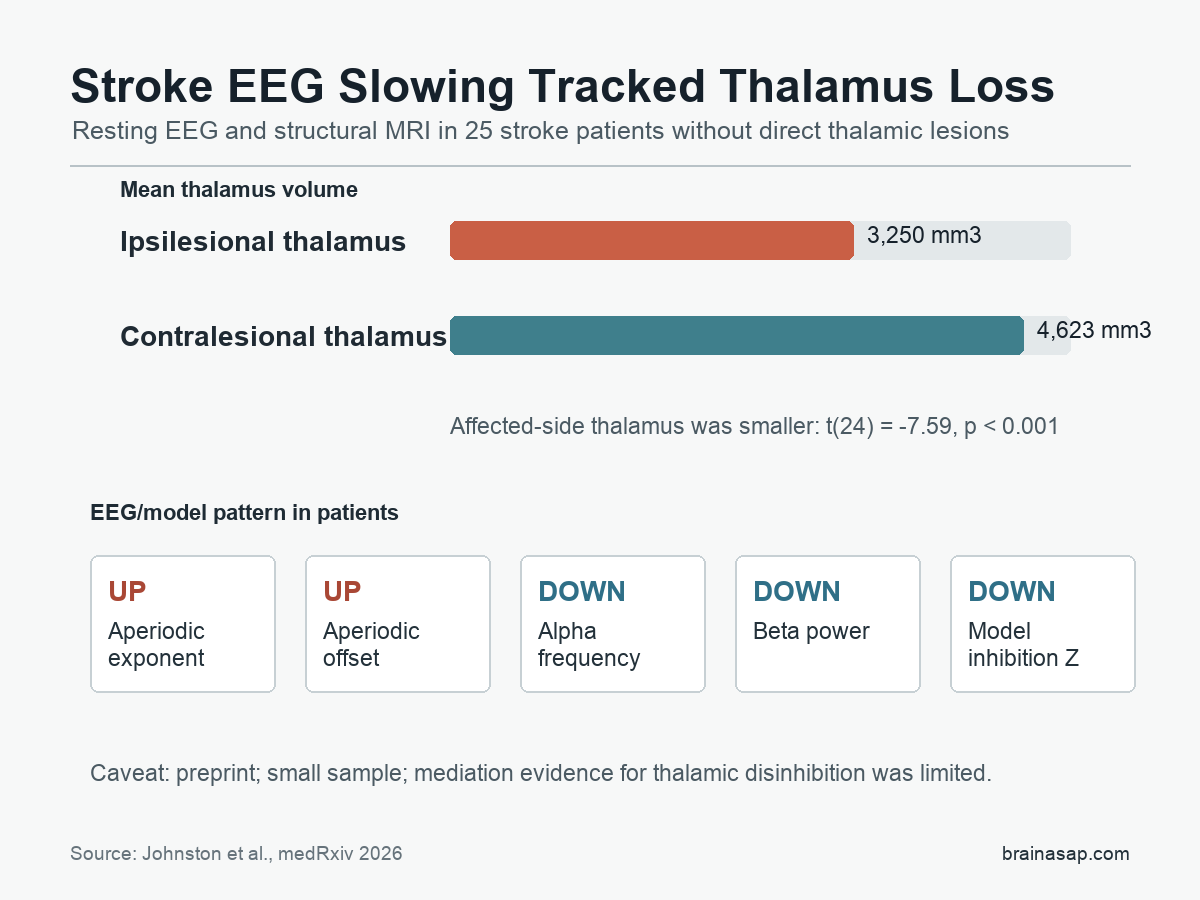
- EEG slowing was multi-part: Stroke patients showed higher aperiodic exponent and offset, lower alpha frequency, reduced beta power, and model-estimated thalamic disinhibition.
- Smaller ipsilesional thalamus: The thalamus on the stroke-affected side averaged 3,250 mm3 versus 4,623 mm3 on the opposite side.
- Preprint caveat: The study supports a biomarker hypothesis, but it was small, not peer reviewed, and did not show a significant link between thalamus volume and available motor/NIHSS scores after correction.
Source: medRxiv (2026) | Johnston et al.
Stroke EEG studies often describe a shift toward slower brain rhythms. This preprint argues that the phrase neural slowing hides several measurable changes, and that many of those changes may point back to the thalamus.
The thalamus is a deep brain relay that helps coordinate cortical activity. In this study, the thalamus itself was not directly hit by the stroke lesion, but the thalamus on the stroke-affected side was smaller and its volume tracked several EEG abnormalities.
EEG Slowing Was Split Into Specific Signal Features
The researchers analyzed 3 minutes of awake resting-state EEG from a high-density 256-electrode system. They used spectral parameterization to separate oscillatory features from the aperiodic background, a broad component of the power spectrum that can make brain activity look shifted toward lower frequencies.
A slower-looking EEG trace can come from more than one source. The stroke group showed a combined pattern rather than one simple rhythm change:
- Aperiodic exponent and offset: Both were elevated across the scalp, meaning the non-oscillatory background was steeper and higher.
- Alpha frequency: The alpha peak was lower in patients, consistent with genuine alpha slowing.
- Beta power: Beta-band power was reduced in the stroke group.
- Model parameter Z: A corticothalamic model estimated lower intrathalamic inhibitory feedback, interpreted in the paper as thalamic disinhibition.
A multivariate analysis separated patients from controls with one significant latent variable (s = 9.091, p = 0.026). The pattern was still broadly present when age was handled as a control issue.
The Ipsilesional Thalamus Was Smaller Despite No Direct Lesion
The patient sample was deliberately filtered to avoid primary thalamic injury. Participants were excluded if the lesion mask overlapped the thalamus, if the imaging suggested a thalamic void, or if the vascular-territory pattern suggested infarct involvement in thalamus-supplying branches.
Even with those exclusions, the thalamus on the affected side was smaller. Mean ipsilesional thalamus volume was 3,250 mm3, compared with 4,623 mm3 on the contralesional side.
The raw side-to-side comparison was statistically strong (t(24) = -7.59, p < 0.001).
The normalized measure told the same story. Ipsilesional thalamus normative deviation averaged -6.75, versus -4.30 contralesionally. That comparison was also significant (t(24) = -7.75, p < 0.001).
Thalamus Volume Predicted Most Slowing Features Better Than Lesion Size
The key analysis asked whether thalamus volume lined up with the EEG and model features. The multivariate model included infarct volume, time since stroke, Upper Extremity Fugl-Meyer score, and NIH Stroke Scale score.
Reduced ipsilesional thalamus volume was associated with a pattern that included higher aperiodic exponent and offset, lower alpha frequency, and lower model-estimated intrathalamic inhibition. The report said thalamus volume was a stronger predictor of those features than overall lesion size or time since stroke onset.
Beta power was the exception. It was lower in stroke patients than controls, but it did not show the same clear relationship with thalamus volume.
The biomarker claim is therefore narrower: secondary thalamic degeneration may explain part of post-stroke slowing, not every EEG abnormality after stroke.
The Mechanism Claim Was Weaker Than the Biomarker Claim
The study supports a relationship between secondary thalamic degeneration and broad EEG slowing. It is less definitive about the exact mechanism linking the two.
The analysis tested whether reduced model-estimated thalamic inhibition statistically mediated the relationship between thalamus volume and spectral slowing. That mediation test did not pass a conventional two-tailed 0.05 threshold in the main analysis.
Several limits make the mechanism harder to settle:
- Small sample: The final analysis included 25 patients and 17 controls, which limits subgroup and mediation power.
- Lesion heterogeneity: Different lesion locations may produce similar scalp-level slowing through partly different routes.
- EEG frequency limits: EEG is more vulnerable to contamination above 15 Hz than some MEG approaches, which may affect beta and model-parameter estimates.
- Single thalamus measure: This study used thalamus volume deviation rather than a richer multimodal thalamus injury panel.
The Result Points to an Accessible Stroke Biomarker
The accessibility signal is straightforward. EEG and structural T1-weighted MRI are easier to obtain than many advanced imaging or magnetoencephalography measures.
If replicated, a combined EEG-plus-MRI marker could help researchers stratify stroke patients by underlying brain-network injury rather than lesion location alone.
The finding should not be used to guide clinical care yet. The paper is a non-peer-reviewed medRxiv preprint, and the available motor and neurological impairment scores did not significantly correlate with thalamus volume after correction for infarct volume.
Still, the study gives a concrete interpretation of an old EEG observation. Post-stroke neural slowing may be more than a vague sign of injured brain activity.
In this sample, several parts of that slowing tracked a measurable secondary injury process in the thalamus.
Citation: DOI: 10.64898/2026.06.29.26356697. Johnston PR et al. Large-scale neural slowing measured with electroencephalography indexes secondary thalamic degeneration in stroke. medRxiv. 2026.
Study Design: Secondary analysis of resting-state EEG, structural MRI, and corticothalamic modeling in stroke patients and controls.
Sample Size: 25 stroke patients with motor impairment and 17 controls.
Key Statistic: Ipsilesional thalamus volume averaged 3,250 mm3 versus 4,623 mm3 contralesionally (t(24) = -7.59, p < 0.001).
Caveat: This is a preprint with a small sample, no direct clinical-use test, and limited evidence for thalamic disinhibition as the causal mediator.