TL;DR: A 2026 review in International Journal of Molecular Medicine mapped how exercise and fluoxetine overlap in Alzheimer’s disease mechanisms such as mitochondrial quality control, oxidative stress, inflammation, and neuroplasticity, but clinical combination benefits remain unproven.
Key Findings
- Review article, not trial: Wu and Li synthesized mechanistic evidence on exercise and fluoxetine in Alzheimer’s disease rather than testing a combined intervention in patients.
- Mitochondrial focus: Exercise was described as supporting mitochondrial biogenesis, mitophagy, energy metabolism, and mitochondrial quality control through pathways including AMPK and PGC-1alpha signaling.
- Shared inflammation targets: Exercise and fluoxetine were both discussed as potential modulators of oxidative stress, NLRP3-related inflammation, and neuroimmune signaling in AD models.
- Neuroplasticity overlap: The review emphasized BDNF, CREB, synaptic plasticity, and cerebrovascular regulation as pathways where exercise and fluoxetine partly overlap.
- Combination uncertainty: The authors highlighted possible synergy but also possible antagonism, especially if fluoxetine interferes with adaptive stress signaling induced by exercise.
Source: International Journal of Molecular Medicine (2026) | Wu and Li
Exercise is one of the most durable non-drug candidates in Alzheimer’s disease research because it affects metabolism, vascular function, inflammation, and synaptic plasticity at the same time. Fluoxetine, a selective serotonin reuptake inhibitor, is more familiar as an antidepressant but has also been studied in Alzheimer’s models.
This review asks whether those two interventions share enough biology to support combined strategies. The answer is cautious: exercise and fluoxetine overlap in several Alzheimer’s pathways, but overlap does not prove that the pair works better together in patients.
Exercise Targets Multiple Alzheimer’s Disease Pathways
The review describes Alzheimer’s disease as a disorder involving amyloid-beta deposition, tau pathology, synaptic dysfunction, neuronal loss, mitochondrial damage, oxidative stress, and neuroinflammation. Exercise is relevant because it can act across several of those domains in preclinical and clinical research.
The most important exercise-related pathways include:
- Mitochondrial biogenesis: Exercise can activate AMPK and PGC-1alpha-related signaling, which supports mitochondrial renewal and energy metabolism.
- Mitochondrial quality control: Exercise supports mitophagy and autophagy-lysosome pathway activity in the evidence reviewed, helping cells clear damaged mitochondria.
- Antioxidant defense: Regular physical activity can strengthen defenses against reactive oxygen species and redox imbalance.
- Synaptic plasticity: Exercise has been linked to BDNF and CREB signaling, both relevant to learning, memory, and synapse maintenance.
Those mechanisms are not isolated. In Alzheimer’s models, energy metabolism, inflammation, synaptic function, and protein clearance often interact, so a multi-pathway intervention can be biologically plausible even when any single pathway is incomplete.
Fluoxetine Has More Than Mood Targets in AD Models
Fluoxetine is a selective serotonin reuptake inhibitor used clinically for depression and related conditions. The review focuses on its possible Alzheimer’s-related effects beyond mood, especially in preclinical models.
The authors describe fluoxetine as potentially influencing mitochondrial homeostasis, oxidative stress, neuroinflammation, autophagy, and neuroplasticity. Some cited work suggests possible effects on amyloid-beta metabolism and tau-related pathways, but the review does not establish fluoxetine as a disease-modifying Alzheimer’s treatment.
That distinction is important. A drug can shift molecular markers in a model without producing a reliable clinical effect in patients with Alzheimer’s disease.
The review’s fluoxetine discussion centers on four possible domains:
- Serotonin signaling: SSRI activity can influence mood, stress biology, and downstream neuroplasticity pathways.
- BDNF and CREB: Fluoxetine is discussed alongside neurotrophic signaling linked to synaptic resilience.
- Inflammation control: Some preclinical findings connect fluoxetine with reduced inflammatory signaling.
- Autophagy and redox balance: The drug is discussed as a potential influence on cellular cleanup and oxidative-stress systems in AD models.
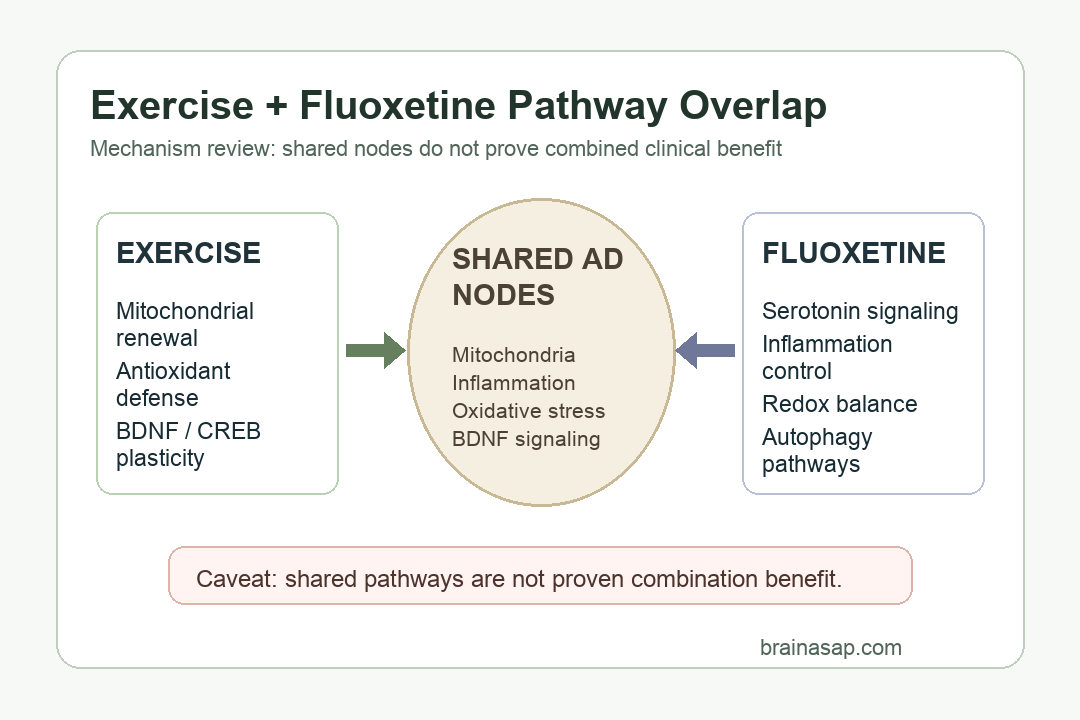
Shared Nodes Include Mitochondria, Inflammation, and BDNF
The review’s central value is its pathway map. Exercise and fluoxetine are both discussed around mitochondrial quality control, oxidative stress, neuroinflammation, and BDNF-related plasticity.
Those shared nodes make a combined intervention plausible in theory. Exercise can create repeated physiological stress that drives adaptation, while fluoxetine can influence serotonin-linked neuroplasticity and inflammatory signaling.
The review also describes evidence from gene-expression and network analyses. In one cited analysis, exercise and fluoxetine were both predicted to reverse parts of Alzheimer’s-related dysregulated gene expression, with a combined intervention predicted to reverse a larger gene set than either intervention alone.
That kind of prediction is hypothesis-generating. It can prioritize pathways and experimental designs, but it cannot tell patients whether adding fluoxetine to exercise will slow cognitive decline.
Fluoxetine Interaction With Exercise Adaptation Remains Uncertain
The review does not treat combination therapy as automatically additive. One concern is that the benefits of exercise often depend on repeated moderate physiological stress followed by adaptation.
If a medication changes stress-response signaling, serotonin tone, mitochondrial responses, or inflammation too strongly, the adaptive response to exercise can shift. The authors discuss several conditions that shape whether the interaction is helpful or harmful:
- Dose: Fluoxetine effects can differ at low, standard, or high exposure levels.
- Timing: Medication timing relative to exercise can affect acute and long-term signaling.
- Exercise intensity: Mild, moderate, and strenuous exercise can produce different stress and recovery profiles.
- Disease stage: Preclinical AD, mild cognitive impairment, and established dementia are unlikely to respond the same way.
That uncertainty is the main reason the review’s message is not “combine them now.” It is “test the combination carefully, with attention to biology, dose, timing, and patient subgroup.”
Clinical Trials Need Cognitive Outcomes, Not Only Pathway Logic
The translational gap is large. Much of the exercise and fluoxetine evidence discussed in the review comes from animal models, cell studies, molecular pathway work, or indirect clinical observations.
Future human studies would need to measure more than molecular markers. The clinically important outcomes include cognition, daily function, neuropsychiatric symptoms, sleep, adverse effects, adherence, and caregiver burden.
A practical trial would also need to separate several questions:
- Exercise alone: Which exercise dose, intensity, and duration improves Alzheimer’s-related outcomes?
- Fluoxetine alone: Does fluoxetine improve cognition, mood, or disease markers in the selected patient group?
- Combined treatment: Does adding fluoxetine to exercise improve outcomes beyond exercise alone, or does it blunt exercise-linked adaptation?
For now, the review supports a mechanistic research agenda. It does not support using fluoxetine as an Alzheimer’s disease-modifying drug outside normal clinical indications.
Citation: DOI: 10.3892/ijmm.2026.5908. Wu M, Li Y. Exercise and fluoxetine in Alzheimer’s disease: Molecular mechanisms of synergistic and antagonistic effects (Review). International Journal of Molecular Medicine. 2026;58:237.
Study Design: Narrative mechanistic review of exercise, fluoxetine, and Alzheimer’s disease pathways.
Sample Size: No new patient sample; the review synthesizes published preclinical, molecular, and clinical evidence.
Key Statistic: A cited gene-expression analysis predicted that combined exercise and fluoxetine would reverse AD-related expression changes in 549 genes.
Caveat: The review does not prove that exercise plus fluoxetine improves cognition or slows Alzheimer’s progression in patients.