TL;DR: A 2026 preprint posted on medRxiv reported that larger choroid plexus volume on brain MRI was associated with greater disability in multiple sclerosis and with higher white-matter myo-inositol in progressive MS, but the work has not yet been peer reviewed.
Key Findings
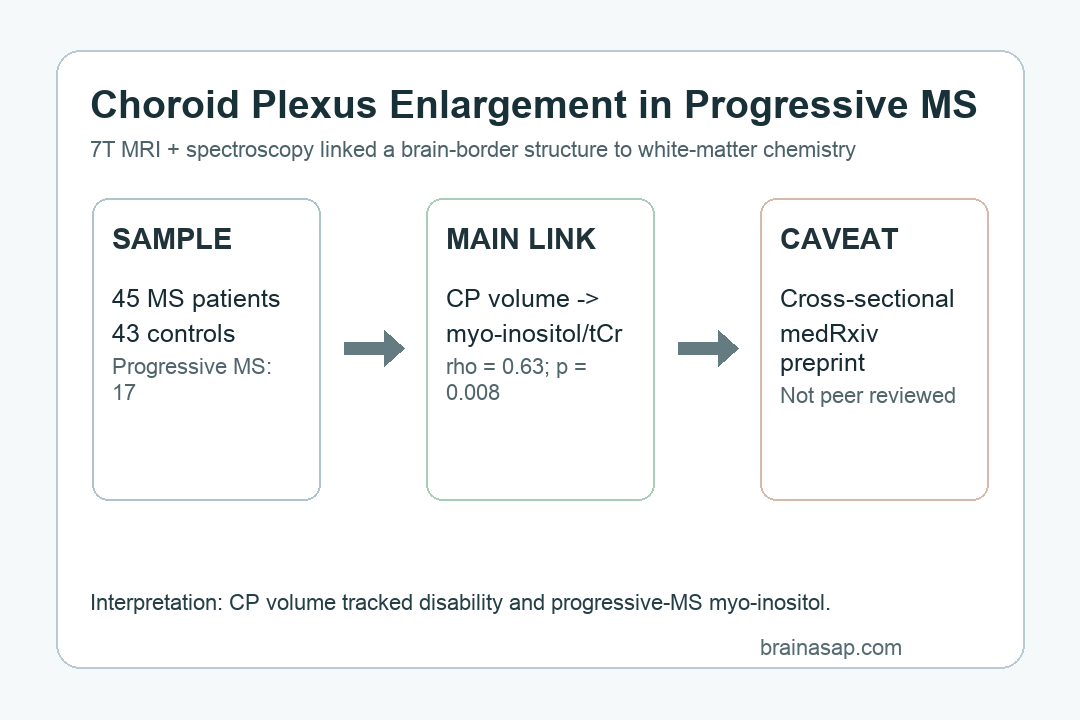
- 88-person imaging sample: Researchers studied 45 people with multiple sclerosis and 43 age- and sex-matched healthy controls using 7T MRI and proton magnetic resonance spectroscopy.
- 17 progressive MS cases: The progressive MS subgroup had a positive association between normalized choroid plexus volume and centrum semiovale white-matter myo-inositol/total creatine (rho = 0.63, p = 0.008).
- No matching RRMS association: The same choroid plexus-to-myo-inositol relationship was not seen in the relapsing-remitting MS subgroup.
- Disability correlation: Across the combined MS cohort, normalized choroid plexus volume correlated with Expanded Disability Status Scale scores (rho = 0.40, p = 0.006).
- White-matter metabolic pattern: Myo-inositol was elevated and total N-acetylaspartate was reduced in centrum semiovale white matter across MS phenotypes compared with controls.
Source: medRxiv (2026) | Senthil et al.
Multiple sclerosis research often separates visible lesion burden from more diffuse tissue injury. This preprint connects those levels by pairing a brain-border structure, the choroid plexus, with magnetic resonance spectroscopy measures inside white matter.
The choroid plexus helps make cerebrospinal fluid and sits at an immune-sensitive boundary between blood, brain, and ventricles. In MS, that location makes it a plausible marker of inflammatory traffic, but a larger structure on MRI does not automatically explain what is happening deeper in white matter.
7T MRI Linked Choroid Plexus Volume to Progressive MS Metabolism
Researchers used ultra-high-field 7T MRI plus proton magnetic resonance spectroscopy, a method that estimates chemical signals inside selected brain regions. The spectroscopy voxels were placed in the posterior cingulate cortex and the centrum semiovale white matter, a white-matter region vulnerable to MS-related injury.
The study included three comparison groups:
- Relapsing-remitting MS: 28 participants, with a mean age of 50.1 years and median EDSS score of 2.
- Progressive MS: 17 participants, with a mean age of 53.6 years and median EDSS score of 4.5.
- Healthy controls: 43 age- and sex-matched people without MS, used as the metabolic comparison group.
The subgroup design fits the biology because progressive MS and relapsing-remitting MS can have different inflammatory and degenerative patterns. A single combined MS analysis could miss a relationship that appears mainly in progressive disease.
The main progressive-MS result was specific: normalized choroid plexus volume was associated with CSWM myo-inositol/total creatine in the progressive subgroup. Myo-inositol is often interpreted as a glial or astrocytic marker in spectroscopy studies, while total creatine is commonly used as a reference signal.
Myo-Inositol Was Higher While N-Acetylaspartate Was Lower
The metabolic pattern was not only about the choroid plexus. In centrum semiovale white matter, people with MS showed higher myo-inositol and lower total N-acetylaspartate than controls.
Those two measures point in different but complementary directions. Myo-inositol can rise when glial activation or osmotic stress is present, while N-acetylaspartate is commonly treated as a marker related to neuronal or axonal integrity.
The strongest practical interpretation is a paired white-matter pattern:
- Glial activation marker: Elevated myo-inositol suggests white matter may be showing an inflammatory or reactive glial signature beyond visible lesions.
- Neuroaxonal compromise marker: Reduced total N-acetylaspartate suggests the same region may also carry evidence of axonal stress or loss.
- Progressive MS link: The choroid plexus association with myo-inositol appeared in progressive MS, where smoldering white-matter pathology is a central concern.
The preprint does not show that choroid plexus enlargement causes the metabolic changes. It shows that people with larger choroid plexus volume tended to have higher white-matter myo-inositol in the progressive subgroup.
Choroid Plexus Volume Also Tracked MS Disability Scores
Across all 45 people with MS, normalized choroid plexus volume correlated with the Expanded Disability Status Scale (EDSS), a clinician-rated scale often used to summarize MS disability. The reported correlation was rho = 0.40, with p = 0.006.
That is not a diagnostic threshold. It is a group-level association suggesting that choroid plexus volume may carry information about disease severity alongside other MRI and clinical measures.
The disability and function measures also explain why the subgroup analysis is clinically relevant. Progressive MS participants had worse average walking and hand-function measures than healthy controls, and their median EDSS score was higher than the relapsing-remitting group.
For MS biomarker work, the finding is more specific than choroid plexus size alone. Larger normalized choroid plexus volume lined up with both EDSS disability and a white-matter glial-metabolism marker.
Single-Voxel Spectroscopy Limits the MS Biomarker Claim
The study is promising because it combines choroid plexus anatomy with tissue chemistry, but several limits keep the claim narrow. The most important limit is that this was a cross-sectional preprint, so the direction of the relationship cannot be settled.
The main constraints are straightforward:
- Small progressive subgroup: The progressive MS analysis rested on 17 people, which makes replication important.
- Single-voxel spectroscopy: Researchers sampled the posterior cingulate cortex and centrum semiovale white matter rather than mapping the whole brain.
- Mixed progressive phenotype: Primary and secondary progressive MS were combined, even though those forms may differ biologically.
- No causal timing: The design cannot show whether choroid plexus enlargement precedes, follows, or merely accompanies white-matter metabolic change.
Those limits do not erase the result. They define the next test: larger longitudinal studies that measure choroid plexus volume, whole-brain spectroscopy, lesion evolution, and disability change over time.
Choroid Plexus Imaging May Add Brain-Border Context in MS
The choroid plexus is attractive as an MS marker because it is visible on routine structural MRI and sits at a biologically relevant immune interface. If future studies replicate the association, choroid plexus volume could help identify a subgroup with more active periventricular or white-matter glial pathology.
The finding should not be read as a treatment target yet. The current data support a biomarker hypothesis: choroid plexus enlargement, white-matter myo-inositol, and MS disability may be connected in progressive disease.
That is enough to make the study worth following, especially because progressive MS still needs better markers of smoldering inflammation and neuroaxonal injury. It is not enough to change clinical care before peer review and independent replication.
Citation: DOI: 10.64898/2026.06.29.26356824. Senthil et al. Choroid Plexus Enlargement is Associated with Disease Severity and Elevated White Matter Myo-inositol in Progressive Multiple Sclerosis. medRxiv. 2026.
Study Design: Cross-sectional 7T MRI and proton magnetic resonance spectroscopy preprint.
Sample Size: 45 people with multiple sclerosis and 43 healthy controls.
Key Statistic: In progressive MS, choroid plexus volume correlated with centrum semiovale white-matter myo-inositol/total creatine (rho = 0.63, p = 0.008).
Caveat: This is a non-peer-reviewed preprint with a small progressive MS subgroup and no causal timing.