TL;DR: A 2026 case study in International Medical Case Reports Journal described a 42-year-old man whose chronic insomnia improved after celiac disease was diagnosed and treated with a gluten-free diet, but the report cannot prove gluten exposure caused the sleep problem.
Key Findings
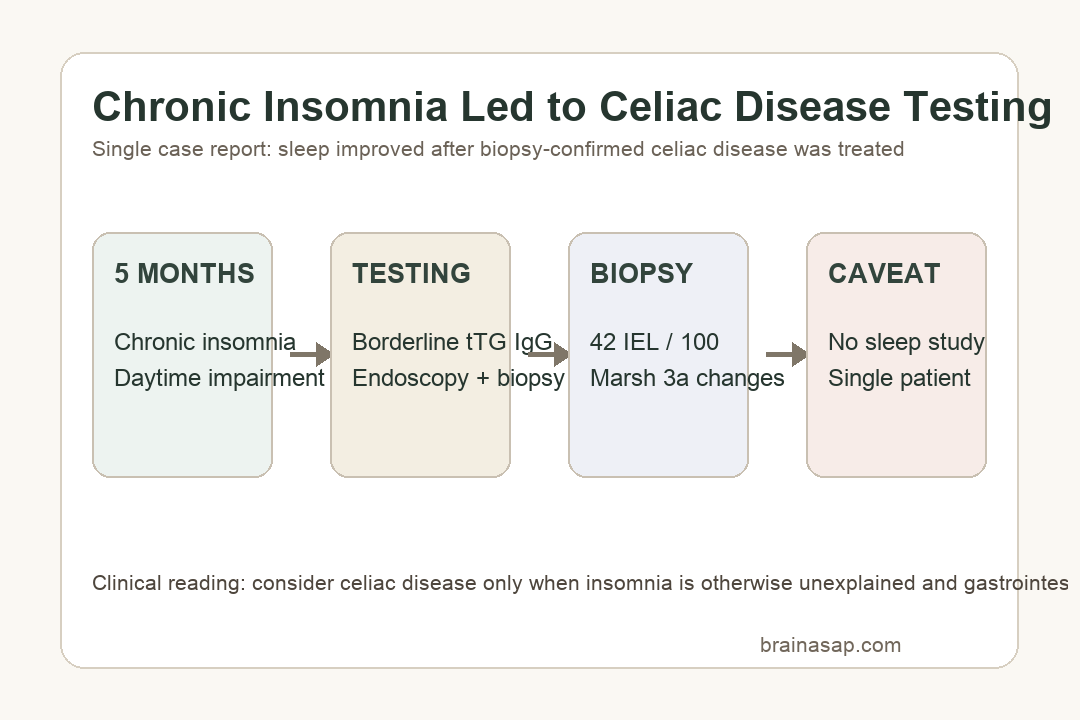
- 5 months of insomnia: The patient reported persistent difficulty initiating and maintaining sleep, severe nocturnal restlessness, daytime fatigue, impaired concentration, irritability, and psychological distress.
- Subtle gut symptoms: He had chronic mild abdominal distension and discomfort, plus a predominantly wheat-based diet, despite no classic severe malabsorption presentation.
- Borderline antibody result: Tissue transglutaminase IgG was borderline elevated at 0.70 kU/L, while deamidated gliadin peptide IgG was negative.
- Biopsy-confirmed celiac disease: Duodenal biopsies showed Marsh-Oberhuber type 3a changes, including partial villous atrophy and 42 intraepithelial lymphocytes per 100 enterocytes.
- Symptoms improved after diet change: Insomnia and gastrointestinal symptoms improved within weeks of starting a strict gluten-free diet, but the report lacked polysomnography, actigraphy, rating scales, and formal psychiatric assessment.
Source: International Medical Case Reports Journal (2026) | Mohamud et al.
Insomnia is common enough that a single unusual medical explanation should be handled carefully. This case report is useful because it shows how a sleep complaint can lead clinicians toward a gastrointestinal diagnosis when the patient also has subtle abdominal symptoms.
The report is not evidence that most chronic insomnia is caused by celiac disease. It is evidence that celiac disease can remain clinically quiet enough that sleep symptoms become the main reason a patient seeks care.
Chronic Insomnia Was the Main Celiac Disease Complaint
The patient was a 42-year-old man seen in an outpatient neurology clinic in Mogadishu, Somalia. His main complaint was 5 months of chronic insomnia that had worsened enough to affect daytime functioning, mood, and quality of life.
He described problems with both sleep onset and sleep maintenance. He also reported daytime fatigue, impaired concentration, irritability, and marked distress from ongoing sleep loss.
Before evaluation, he had already tried common first steps:
- Sleep schedule changes: He tried to keep a consistent sleep routine.
- Environmental changes: He tried to optimize the sleep environment and limit screen exposure before bed.
- Caffeine restriction: He reduced a common sleep-disrupting exposure.
- Over-the-counter sleep aids: Antihistamine-based products did not provide meaningful improvement.
That history made the case more than a brief sleep complaint. The symptom burden was persistent, functionally important, and resistant to low-level self-management.
Borderline tTG IgG Led to Duodenal Biopsy
The diagnostic turn came from details outside the sleep history. The patient had mild chronic abdominal distension and discomfort that he had tolerated for a long time, and his diet was predominantly wheat-based.
Serology showed borderline tissue transglutaminase IgG at 0.70 kU/L. The authors noted that IgG-based testing may be less sensitive and specific than IgA-based celiac serology, so the borderline result needed clinical context rather than automatic dismissal.
Upper gastrointestinal endoscopy found erythematous and edematous mucosa in the first and second portions of the duodenum. Biopsies then provided the stronger diagnostic evidence.
The biopsy findings were specific:
- Partial villous atrophy: The absorptive surface of the small intestine was blunted.
- Crypt hyperplasia: The crypts were elongated with increased mitotic activity.
- Enterocyte flattening: Surface cells lost their normal columnar appearance.
- 42 IEL/100 enterocytes: Intraepithelial lymphocytes exceeded the normal threshold of 25 per 100 enterocytes.
Together, those features fit Marsh-Oberhuber type 3a celiac disease. The sleep complaint did not diagnose celiac disease by itself; the biopsy did.
Gluten-Free Diet Coincided With Sleep Improvement
After diagnosis, clinicians started a strict gluten-free diet. The patient reported marked improvement in both insomnia and gastrointestinal symptoms within weeks.
That time course is clinically notable, but it remains a temporal sequence rather than a controlled experiment. There was no blinded gluten challenge, no repeated objective sleep measurement, and no comparison patient.
The case still gives clinicians a practical checklist when insomnia remains unexplained:
- Ask about quiet gastrointestinal symptoms: Mild bloating, discomfort, or diet-linked symptoms may not be volunteered unless directly asked.
- Review dietary exposure: A wheat-heavy diet can make celiac disease more clinically visible in susceptible people.
- Use confirmatory testing: Borderline serology should not replace endoscopy and biopsy when suspicion remains.
- Track sleep formally when possible: Rating scales, actigraphy, or polysomnography would make future cases easier to interpret.
Single-Case Evidence Cannot Prove Celiac Disease Caused Insomnia
The strongest caveat is the sample size: this is one patient. Chronic insomnia can arise from psychiatric disorders, circadian disruption, medications, pain, restless legs syndrome, sleep apnea, stress, substance use, and many other causes.
The report also lacked several measurements that would strengthen a sleep-focused case. The patient did not undergo polysomnography, actigraphy, validated insomnia rating scales, or a formal psychiatric evaluation.
Those gaps are not minor. Without objective or structured sleep assessment, the improvement after diet change depends mainly on clinical observation and patient report.
Mechanistically, the authors discussed several plausible routes between celiac disease and sleep symptoms:
- Immune activation: Systemic inflammation could affect sleep-regulating brain circuits.
- Micronutrient deficiency: Malabsorption can affect iron, folate, vitamin B12, vitamin D, and magnesium, which may influence sleep or restlessness.
- Gut-brain signaling: Intestinal immune activity and microbiome changes may affect neuropsychiatric symptoms.
Those mechanisms are plausible but not demonstrated in this patient. The case identifies a diagnostic possibility, not a general insomnia explanation.
Unexplained Insomnia May Need Broader Medical Screening
The useful clinical message is narrow: when chronic insomnia is persistent, unexplained, and accompanied by subtle gastrointestinal symptoms, celiac disease can belong in the differential diagnosis.
Broad gluten avoidance should not replace medical evaluation. Celiac diagnosis requires appropriate serology, attention to total IgA status when relevant, and biopsy confirmation in many clinical pathways.
For patients, the case also shows why mentioning mild or long-tolerated symptoms matters during a sleep evaluation. A symptom that seems unrelated to sleep may point clinicians toward the condition that needs testing.
Citation: DOI: 10.2147/IMCRJ.S620742. Mohamud et al. Chronic Insomnia as an Uncommon Manifestation of Celiac Disease: A Case Report. International Medical Case Reports Journal. 2026;19:620742.
Study Design: Single-patient case report with neurology and gastroenterology evaluation.
Sample Size: 1 adult male patient.
Key Statistic: Duodenal biopsy showed 42 intraepithelial lymphocytes per 100 enterocytes, above the normal threshold of 25 per 100 enterocytes.
Caveat: No objective sleep study, validated insomnia scale, formal psychiatric evaluation, or causal rechallenge was reported.