TL;DR: A 2026 pilot study in The British Journal of Psychiatry tested psilocybin-assisted therapy in 21 adult females with anorexia nervosa and found lower Eating Disorder Examination (EDE) symptom scores through 6 months, with large individual variation and no placebo-controlled comparison.
Key Findings
- Single-arm pilot study: Researchers enrolled 21 adult females with anorexia nervosa and gave 3 oral psilocybin sessions alongside psychological support and treatment as usual.
- Dosing sequence: Participants received 1 mg, then 25 mg, then 25 mg of COMP360 psilocybin over 6 weeks, with preparation and integration therapy around each session.
- EDE symptoms decreased: Global clinician-rated Eating Disorder Examination scores fell from 3.2 at baseline to 2.1 at 6 months (p < 0.0001, d = 0.98).
- Motivation improved: Readiness and Motivation Questionnaire precontemplation scores, a measure of lower readiness to change, improved across follow-up and remained lower at 12 months (p = 0.0017, d = 0.65).
- Safety needs careful reading: Headache, nausea, and dizziness were common; 2 later suicide attempts in 1 participant were reported as serious adverse events and judged unlikely to be related to psilocybin.
Source: The British Journal of Psychiatry (2026) | Douglass et al.
Psilocybin-assisted therapy is being tested in several psychiatric conditions, but anorexia nervosa is a difficult test case because the disorder can be medically fragile, long-lasting, and resistant to treatment.
This small pilot established feasibility and found lower Eating Disorder Examination scores through 6 months, but without a placebo group it cannot show that psilocybin caused the improvement.
21 Women Received 3 Psilocybin Sessions Over 6 Weeks
Researchers recruited adult females aged 21 to 65 with a primary DSM-5 diagnosis of anorexia nervosa that had likely lasted more than 3 years. The enrolled group was clinically ill: mean body mass index (BMI) was 16.4 kg/m2, and mean estimated illness duration was 10.8 years.
The study used a single-arm, single-blind, fixed-order design. That means every participant received the same dose sequence rather than being randomized to psilocybin or placebo.
The treatment structure was intensive:
- Dose 1: 1 mg psilocybin, used as the initial session in the fixed sequence.
- Dose 2: 25 mg psilocybin, given 2 weeks later.
- Dose 3: 25 mg psilocybin, again 2 weeks later.
- Therapy support: Each dosing day was paired with preparation and integration sessions, while participants continued usual eating-disorder treatment.
- Follow-up: In-person assessment continued through 6 weeks, with remote monthly follow-ups through 6 months and a final remote 12-month follow-up.
Retention was high. Of 21 enrolled participants, 20 completed the active study period, producing a 95.2% retention rate.
Clinician-Rated Eating Disorder Scores Fell Through 6 Months
The main symptom outcome was the Eating Disorder Examination (EDE), a clinician-administered interview that measures eating-disorder psychopathology. Global EDE scores decreased significantly over time.
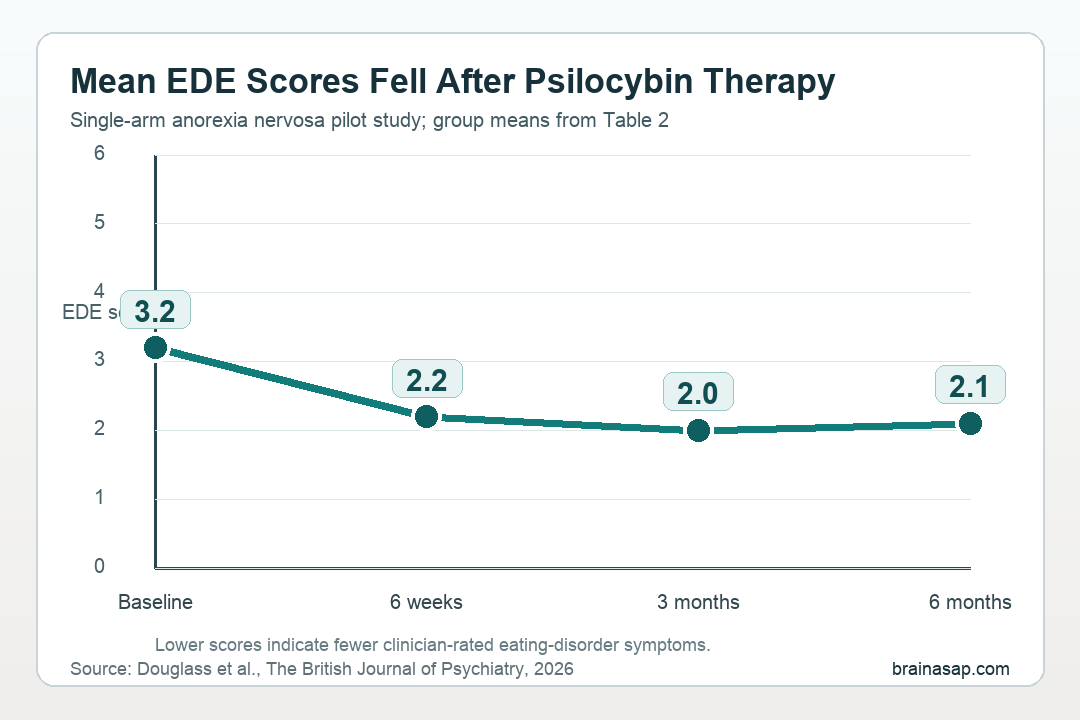
The mean global EDE pattern was:
- Baseline: 3.2, with a standard deviation of 1.0.
- Final visit at 6 weeks: 2.2, a 1.0-point reduction from baseline.
- 3-month follow-up: 2.0, the lowest mean value reported for the clinician-rated outcome.
- 6-month follow-up: 2.1, still significantly below baseline (p < 0.0001, d = 0.98).
All but 2 completers showed lower global EDE scores between baseline and the final visit. The study also reported improvements in dietary restraint, eating concerns, shape concerns, and weight concerns, although the weight-concern improvement did not remain statistically significant at 6 months.
Motivation to Change Improved, but Dose Effects Were Not Clear
The study also tracked Readiness and Motivation Questionnaire (RMQ) precontemplation scores. In this context, lower precontemplation means participants were moving away from low readiness to change and toward greater recognition of the disorder and need for recovery.
RMQ precontemplation scores improved significantly across follow-up. The reduction remained significant at 12 months (p = 0.0017, d = 0.65), with the largest reported reductions around the 2- and 3-month follow-ups.
The dose-specific interpretation is weaker. Researchers did not find a significant main effect of dose on short-term change in either self-reported EDE-Q scores or RMQ precontemplation scores.
The protocol bundled several active ingredients:
- Psilocybin exposure: 1 low-dose session and 2 sessions at 25 mg.
- Psychological support: Preparation and integration sessions around each dose.
- Treatment as usual: Participants remained under specialist eating-disorder care or private therapy.
- Time and attention: The trial involved about 50 hours of therapeutic contact over a compressed period.
Without a randomized control group receiving matched therapy without active psilocybin, the trial cannot separate the drug effect from therapy, expectancy, clinical attention, natural fluctuation, or other post-study changes.
Adverse Events Were Common but Mostly Mild or Moderate
Every participant reported at least 1 adverse event, with 107 total adverse-event reports. Most were classified as mild or moderate, and tranquillising medication was not required for any participant.
The most common events were headache, reported by 18 participants, and nausea, reported by 12 participants. Dizziness, migraine, light-headedness, anxiety, gastrointestinal symptoms, and other events were also recorded.
The safety data need careful interpretation. 1 participant attempted suicide 2 times approximately 7 and 9 months after the final study visit.
Investigators reported those events as serious adverse events and judged them unlikely to be related to the investigational psilocybin product.
For a population with anorexia nervosa, that distinction is clinically important: the trial found the protocol feasible and generally tolerated under strict screening and specialist monitoring, not that psilocybin therapy is broadly safe outside a controlled medical research setting.
Small, Homogeneous, Non-Randomized Design Limits the Claim
The supported claim is narrow. In this carefully screened group, the protocol was feasible, retention was high, and symptom measures improved after a structured psilocybin-assisted therapy program.
The main limitations are direct:
- No placebo control: There was no separate matched group receiving therapy without active psilocybin.
- Fixed dose order: Everyone received 1 mg initially, then 25 mg, then 25 mg, so dose order and time cannot be separated cleanly.
- Small sample: The study enrolled 21 participants and treated analyses as exploratory.
- Homogeneous cohort: The group was mostly highly educated White females, which limits generalization.
- Strict screening: Exclusions and medical oversight mean the results should not be extrapolated to medically unstable or unsupervised settings.
Those limits define the finding. The study supports larger randomized trials of psilocybin-assisted therapy for anorexia nervosa.
The next useful designs would match psychological support across arms and follow participants long enough to test durability.
Citation: DOI: 10.1192/bjp.2026.10687. Douglass HM, Spriggs MJ et al. Psilocybin therapy for adult females with anorexia nervosa: pilot study. The British Journal of Psychiatry. 2026;1-9.
Study Design: Single-arm, single-blind, within-individual pilot study of 3 oral psilocybin sessions plus psychological support and treatment as usual.
Sample Size: 21 adult females with anorexia nervosa; 20 completed the active study period.
Key Statistic: Mean global EDE score decreased from 3.2 at baseline to 2.1 at 6 months (p < 0.0001, d = 0.98).
Caveat: No randomized placebo-control group, small homogeneous sample, fixed dose order, strict screening, and 2 later serious adverse events in 1 participant mean the findings are preliminary.