TL;DR: A 2026 qualitative study in the Journal of Substance Use and Addiction Treatment found that syringe service programs helped people receive buprenorphine quickly, but participants said precipitated withdrawal and limited at-home initiation guidance made treatment harder to start and continue.
Key Findings
- 12 exit interviews: Researchers interviewed people after a randomized trial of buprenorphine treatment through syringe service programs or enhanced referral to a community health center.
- Same-day access helped: Participants in the onsite syringe-service arm reported seeing a provider and receiving a buprenorphine prescription on the day they enrolled.
- Withdrawal complicated initiation: Precipitated withdrawal led some participants to delay, stop, or avoid starting buprenorphine.
- SSP trust was central: Participants described syringe service programs as familiar, affirming, and less stigmatizing than many prior care settings.
- High-touch support was needed: The paper supported a low-threshold, high-touch model that pairs rapid prescribing with check-ins, peer support, and clearer initiation guidance.
Source: Journal of Substance Use and Addiction Treatment (2026) | McGill et al.
Syringe service programs are often easier to reach than conventional clinics for people who inject drugs. They can provide sterile supplies, harm-reduction counseling, social services, and, in some programs, medication treatment for opioid use disorder.
The 2026 study focused on a narrow but practical question: when buprenorphine starts in that setting, what helps people begin treatment, and what still gets in the way?
Syringe Service Programs Made Buprenorphine Easier to Reach
The study drew on exit interviews from a randomized trial in New York City. In the parent trial, 97 syringe-service participants were assigned either to onsite buprenorphine treatment initiation at a syringe service program or to enhanced referral to a community health center.
This qualitative analysis included 12 participants who completed semi-structured exit interviews after the trial. Most were middle-aged men, and 50% identified as Latino.
- Onsite model: Buprenorphine treatment was initiated at a syringe service program.
- Referral model: Participants received enhanced referral to a community health center with an office-based buprenorphine program.
- Interview focus: Researchers asked about provider experiences, starting buprenorphine, prior treatment, and continuing care.
- Analysis: Four researchers coded transcripts and identified recurring themes through thematic analysis.
All interviewees from the onsite arm reported meeting with a provider and receiving a buprenorphine prescription the same day they enrolled. Participants described that as easier than traveling to a separate clinic, waiting for appointments, or navigating a less familiar system.
Same-Day Prescriptions Did Not Solve the Initiation Step
Rapid access was valuable, but the paper did not treat prescription access as the whole answer. Several participants wanted more support when they started taking buprenorphine at home.
Buprenorphine can trigger precipitated withdrawal if someone takes it too soon after opioids, especially in a fentanyl-contaminated drug supply. Participants described fear, confusion, severe symptoms, and uncertainty about when it was safe to begin.
The core mismatch was clear: low-threshold care reduced the barrier to getting medication, but starting the medication still required timing, confidence, and support.
Four Themes Explained Why Support Mattered
The researchers identified four main themes around buprenorphine initiation. Together, they point to care that is accessible but still personal enough to help people through the hardest first days.
- Onsite access helped: Syringe-service treatment made prescriptions easier to obtain, but some participants wanted more guidance after the visit.
- Withdrawal was a major barrier: Precipitated withdrawal affected people in both the onsite and referral arms and could stop treatment continuation.
- The SSP felt affirming: Participants often described syringe service programs as familiar, welcoming, and less stigmatizing than prior medical settings.
- Relationships affected initiation: Respect, time, and trust with clinicians or staff shaped whether participants felt prepared to start treatment.
The setting itself had mixed effects. The same open, familiar environment that made the syringe service program approachable could also be distracting for some people trying to start recovery while others nearby were still discussing or using substances.
Even so, the authors noted that this did not prevent the onsite-arm participants from starting buprenorphine treatment. The bigger clinical problem was not the existence of the syringe service setting; it was the need for stronger initiation support.
Precipitated Withdrawal Was the Main Clinical Friction
Participants described precipitated withdrawal as a reason for not starting buprenorphine after receiving a prescription, stopping after severe symptoms, or switching treatment paths.
The paper reported that none of the participants who went through severe precipitated withdrawal during initiation remained on buprenorphine at the interview, although some had stopped opioid use entirely.
The problem was especially difficult for participants experiencing homelessness. Starting buprenorphine can require waiting through opioid withdrawal before the first dose, and some participants did not have a stable place to be sick long enough to begin.
- At-home uncertainty: Some participants were unsure when symptoms meant it was safe to take the first dose.
- Fentanyl context: Participants and authors described fentanyl in the unregulated opioid supply as making initiation harder to time.
- Support gap: Participants suggested check-ins from clinicians, peers, or staff while they were starting at home.
- Supervision needs: Some preferred home initiation, while others said a more supervised setting would have helped.
The Proposed Model Was Low-Threshold and High-Touch
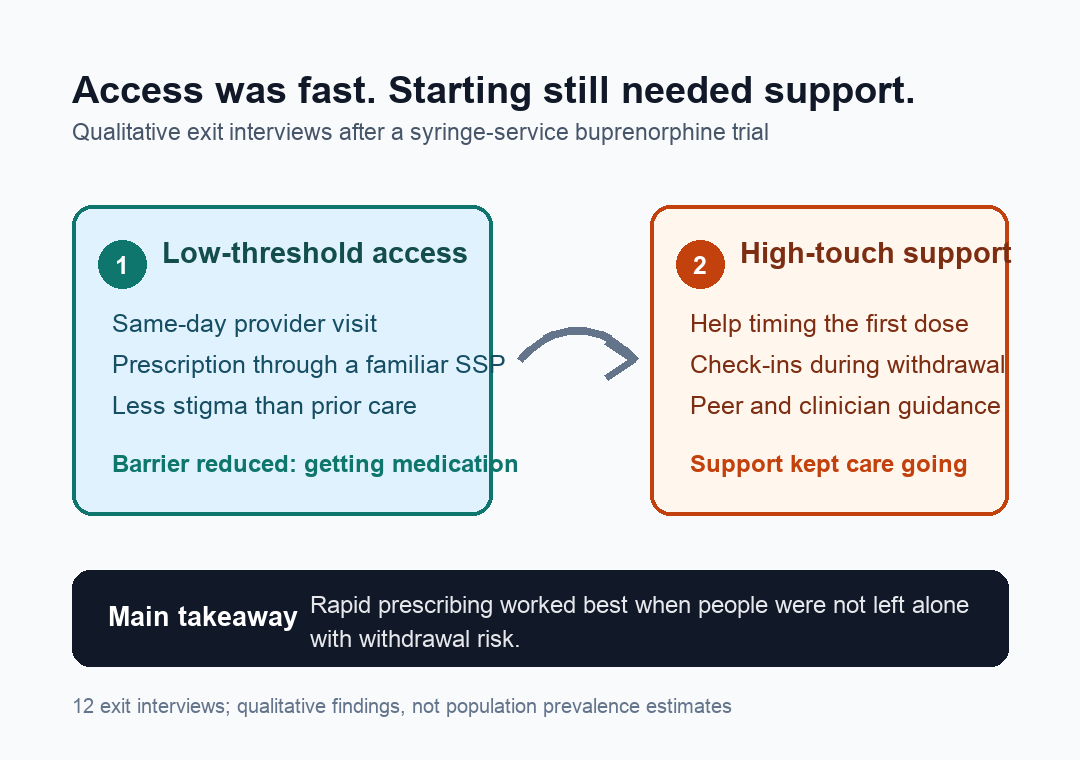
The authors concluded that syringe service programs can be strong venues for buprenorphine treatment, but the model should pair rapid access with more support. They described this as low-threshold, high-touch care.
Low-threshold care means same-day access, flexible visits, and a harm-reduction approach to ongoing opioid use. High-touch care means the person is not left alone with the hardest initiation steps after a prescription is written.
In practical terms, high-touch initiation could include:
- Clinician check-ins: Contacts during the first days to answer dosing and symptom questions.
- Peer support: Help from people who can translate instructions and reduce the power gap of clinical visits.
- Symptom planning: Guidance for nausea, vomiting, diarrhea, anxiety, and other withdrawal symptoms.
- Flexible initiation pathways: Options for at-home starts, supervised starts, or extra support for people without stable housing.
The study was small and qualitative, so it cannot estimate how often each barrier occurs in the broader population. It also sampled people from a randomized trial, which may not fully represent everyone who uses syringe service programs.
Its value is more practical: participants explained why access alone was not enough. For buprenorphine programs in harm-reduction settings, the next improvement may be less about writing the prescription faster and more about helping people get through the first dose safely.
Citation: DOI: 10.1016/j.josat.2026.210027. McGill et al. “It was good because they have a relationship with us:” A qualitative study on low-threshold buprenorphine treatment at syringe services programs. Journal of Substance Use and Addiction Treatment. 2026;189:210027.
Study Design: Qualitative exit-interview study nested within a randomized trial of onsite syringe-service buprenorphine initiation versus enhanced referral.
Sample Size: 12 interviewed participants from a 97-person parent trial.
Key Statistic: Four themes identified rapid prescription access, precipitated withdrawal, affirming syringe-service settings, and provider relationships as central to buprenorphine initiation.
Caveat: The sample was small and trial-based, so the findings describe participant experiences rather than population-level treatment outcomes.