TL;DR: A 2026 randomized trial in BMC Anesthesiology found that adding an esketamine-adjuvanted stellate ganglion block to intraoperative esketamine plus dexmedetomidine reduced early postoperative sleep disturbance after gynecological laparoscopic surgery.
Key Findings
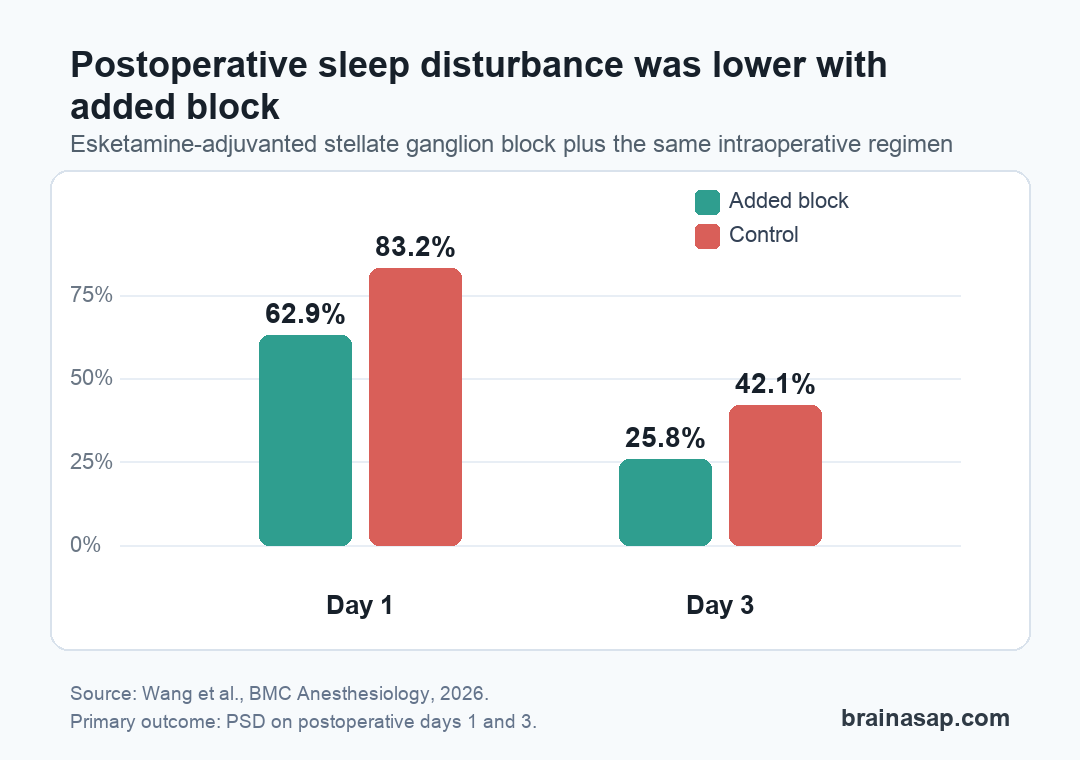
- Sleep disturbance fell on day 1: Postoperative sleep disturbance affected 62.9% of patients in the stellate ganglion block group versus 83.2% in controls.
- The day-3 gap persisted: By postoperative day 3, sleep disturbance was 25.8% with the block versus 42.1% in controls.
- Anxiety was lower early: Day-1 anxiety affected 5.2% of intervention patients versus 17.9% of controls.
- The comparison was incremental: Both groups already received intraoperative esketamine and dexmedetomidine, so the trial tested the added value of the esketamine-adjuvanted block.
- The evidence is short-term: The single-center study used per-protocol analysis and subjective sleep scales, so larger trials with objective sleep measures are still needed.
Postoperative sleep disturbance is common after general anesthesia, and the problem can be especially visible after gynecological laparoscopic surgery. The new trial asked whether a more targeted perioperative sleep strategy could reduce that early disruption.
The answer was yes, but with an important boundary: this was not a test of esketamine alone or stellate ganglion block alone. It tested whether adding a right-sided esketamine-adjuvanted stellate ganglion block improved outcomes on top of the same intraoperative esketamine and dexmedetomidine regimen used in the control group.
Esketamine-Added Stellate Ganglion Block Cut Early Sleep Disturbance
The trial screened 222 patients and randomized 220 adult women scheduled for elective gynecological laparoscopic surgery. After withdrawals and protocol exclusions, 192 patients were included in the per-protocol analysis: 97 in the intervention group and 95 in the control group.
Patients in the control group received intraoperative esketamine at 0.3 mg/kg/h plus dexmedetomidine at 0.2-0.4 micrograms/kg/h. Patients in the intervention group received the same intraoperative regimen, plus an ultrasound-guided stellate ganglion block before anesthesia induction using 1% ropivacaine, esketamine, and saline.
- Control regimen: Intraoperative esketamine plus dexmedetomidine, with multimodal analgesia after surgery.
- Intervention regimen: The same control regimen plus an esketamine-adjuvanted stellate ganglion block before induction.
- Primary outcome: Postoperative sleep disturbance on postoperative days 1 and 3, assessed with the Pittsburgh Sleep Quality Index and Athens Insomnia Scale.
The primary sleep outcome moved in the intervention direction at both follow-ups. On postoperative day 1, postoperative sleep disturbance affected 61 of 97 patients in the intervention group and 79 of 95 patients in the control group.
That corresponds to 62.9% vs. 83.2%, with an odds ratio of 0.343 and a P value of 0.002. By postoperative day 3, the rates were 25 of 97 and 40 of 95, or 25.8% vs. 42.1%.
The Benefit Was Moderate, Not Complete
The day-3 result matters because it shows the separation did not disappear immediately after surgery. The paper also reports a clinically useful framing: the day-3 absolute risk reduction was about 16 percentage points, which the authors described as roughly one prevented case of postoperative sleep disturbance for every six treated patients.
Still, the intervention did not eliminate the problem. Even in the stellate ganglion block group, 25.8% of patients still had postoperative sleep disturbance on day 3. That residual burden is important because it keeps the result from sounding like a cure for postoperative insomnia.
- Sleep scales improved: Day-1 PSQI and AIS scores were lower in the intervention group.
- Early anxiety improved: Day-1 anxiety was 5.2% with the block versus 17.9% in controls.
- Pain did not clearly separate: Resting and movement pain scores did not significantly differ between groups.
- Depression did not clearly separate: Postoperative depression incidence was not significantly different on days 1 or 3.
The anxiety signal is worth noting because esketamine and sympathetic modulation can plausibly affect affective symptoms. But the study did not measure biomarkers or direct neural mechanisms, so the safer reading is that anxiety was a secondary clinical outcome, not proof of how the block worked.
Baseline Risk Factors Still Shaped Postoperative Sleep
Regression analysis identified several independent risk factors for postoperative sleep disturbance. The list included preoperative sleep disturbance, preoperative anxiety, resting pain scores, abdominal drainage placement, and total hysterectomy.
That pattern fits the clinical picture: sleep after surgery is shaped by anesthesia, pain, baseline sleep quality, mood symptoms, surgical stress, and postoperative recovery demands. A nerve block plus anesthetic adjunct can help, but it sits inside a broader perioperative risk system.
The subgroup analysis suggested benefit in patients with preoperative depressive symptoms, but those results should be treated cautiously. The authors explicitly framed the subgroup work as exploratory, and the trial was not powered to turn subgroup findings into firm treatment-selection rules.
The Trial Design Leaves Several Caveats
The main strength is that this was a randomized controlled trial with balanced baseline characteristics. Age, BMI, surgical type, preoperative anxiety and depression scores, and baseline sleep-quality measures were similar between groups.
The main limitations are also clear. The study was conducted at one center, the anesthesiologist performing the block could not be blinded, and the final analysis excluded about 13% of randomized patients after randomization. Because the trial did not include an intention-to-treat analysis, the size of the benefit may be somewhat overestimated.
- Subjective sleep measures: The trial used PSQI and AIS scores rather than polysomnography or actigraphy.
- Short follow-up: Sleep was assessed only during the early postoperative period.
- Single surgical context: The patients were adult women undergoing gynecological laparoscopy, so other procedures need separate testing.
- Mechanism not measured: The paper discusses sympathetic and glutamatergic pathways, but did not directly test them.
Safety findings were reassuring within this sample. One intervention patient developed hoarseness attributed to unintended nerve block, and overall postoperative complication rates did not significantly differ between groups. That does not remove the need for larger safety datasets, but it does mean the sleep signal was not paired with an obvious early complication penalty.
For now, the practical takeaway is narrow and useful: in this single-center trial, an esketamine-adjuvanted stellate ganglion block added to esketamine plus dexmedetomidine reduced early postoperative sleep disturbance after gynecological laparoscopic surgery. The next test is whether that finding holds in multicenter trials with objective sleep tracking and intention-to-treat analysis.
Citation: DOI: 10.1186/s12871-026-04042-0. Wang et al. Esketamine-augmented stellate ganglion block improves postoperative sleep quality after gynecological laparoscopic surgery: a randomized controlled trial. BMC Anesthesiology. 2026.
Study Design: Single-center prospective randomized controlled trial in elective gynecological laparoscopic surgery.
Sample Size: 192 patients in the per-protocol analysis after 220 randomized patients.
Key Statistic: Postoperative sleep disturbance was 62.9% vs. 83.2% on day 1 and 25.8% vs. 42.1% on day 3 with the intervention versus control.
Caveat: The trial used subjective sleep scales, excluded some randomized patients from per-protocol analysis, and needs multicenter confirmation with objective sleep measures.