TL;DR: A 2026 cross-sectional study in Metabolic Brain Disease linked adult attention-deficit/hyperactivity disorder (ADHD) with lower serum SIRT-1, Nrf-2, and HO-1, three redox-regulation markers tied to antioxidant defense.
Key Findings
- 120 adults studied: The analysis compared 60 adults with ADHD against 60 age- and sex-matched healthy controls.
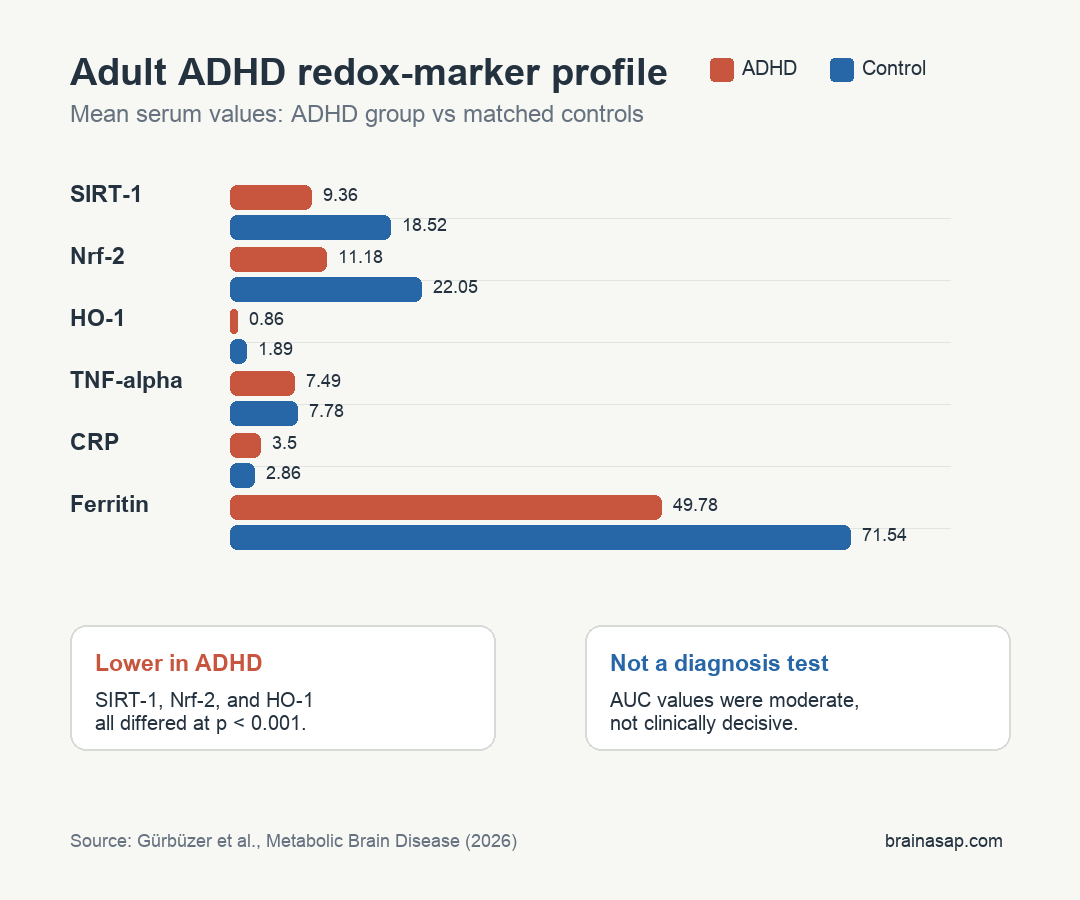
- SIRT-1 was lower: Mean serum SIRT-1 was 9.36 in the ADHD group versus 18.52 in controls, with p < 0.001.
- Nrf-2 and HO-1 were lower: Nrf-2 averaged 11.18 vs 22.05, while HO-1 averaged 0.86 vs 1.89, both with p < 0.001.
- TNF-alpha did not differ: Tumor necrosis factor-alpha was similar between groups, at 7.49 vs 7.78, with p = 0.439.
- Severity correlations were moderate: SIRT-1, Nrf-2, and HO-1 were each negatively correlated with Adult ADHD Self-Report Scale scores, with r values from -0.424 to -0.446.
Source: Metabolic Brain Disease (2026) | Gürbüzer et al.
Attention-deficit/hyperactivity disorder (ADHD) is usually discussed through attention, impulsivity, executive function, and dopamine-related treatment. This study looked at a different layer: whether adults with ADHD show measurable differences in blood markers related to oxidative stress and cellular defense.
The researchers did not test whether these markers cause ADHD. They measured whether the adult ADHD group had a different serum profile than matched controls, then checked whether the same markers tracked symptom severity.
Adult ADHD Was Compared With Matched Healthy Controls
The study enrolled 60 adults diagnosed with ADHD and 60 healthy controls matched by age and sex. ADHD diagnosis was based on structured DSM-5 clinical interviews and the Diagnostic Interview for ADHD in Adults 2.0.
Symptom severity was measured with the Adult ADHD Self-Report Scale (ASRS), a questionnaire used to quantify current adult ADHD symptoms. Blood testing focused on markers that sit in inflammatory or antioxidant-defense pathways.
- SIRT-1: A regulatory protein involved in stress responses, metabolism, and inflammation-related signaling.
- Nrf-2: A transcription factor that helps switch on antioxidant-response genes.
- HO-1: Heme oxygenase-1, an enzyme controlled partly by Nrf-2 and often used as a cellular stress-response marker.
- TNF-alpha: A pro-inflammatory cytokine measured here to test whether a broad inflammatory marker differed between groups.
This design gives a snapshot of group differences. It cannot show whether altered redox regulation begins before ADHD symptoms, follows chronic stress and medication patterns, or reflects a broader metabolic state.
SIRT-1, Nrf-2, and HO-1 Were Lower in Adults With ADHD
The clearest result was a lower antioxidant-defense profile in the ADHD group. Mean serum SIRT-1 was 9.36 in adults with ADHD and 18.52 in controls.
Two related markers showed the same direction. Nrf-2 averaged 11.18 in the ADHD group compared with 22.05 in controls, while HO-1 averaged 0.86 compared with 1.89.
All three comparisons were statistically significant at p < 0.001. The direction is also coherent because the markers sit in related stress-response biology rather than three unrelated lab measurements.
- SIRT-1: About half the control-group mean.
- Nrf-2: Lower by a similar relative margin.
- HO-1: Lower in the same direction as the upstream Nrf-2 marker.
TNF-Alpha Did Not Separate the ADHD and Control Groups
Inflammation did not show a simple one-marker answer. TNF-alpha was 7.49 in adults with ADHD and 7.78 in controls, a nonsignificant difference.
Routine inflammatory and iron-related markers were mixed. CRP was modestly higher in the ADHD group, while ferritin was lower, but the main contrast was not a broad rise in TNF-alpha.
- TNF-alpha: Similar between groups, so the study does not support a simple TNF-alpha ADHD biomarker.
- CRP: Higher in the ADHD group, but the difference was smaller than the redox-marker contrasts.
- Ferritin: Lower in the ADHD group, which may relate to iron biology but needs cautious interpretation.
The inflammatory readout needs that separation because broad inflammation language can get overused. The data favored altered redox-regulatory markers rather than a uniform inflammatory elevation.
Lower Redox Markers Tracked Higher ADHD Symptom Scores
The marker differences were not only group contrasts. Within the sample, lower antioxidant-defense markers were associated with higher ADHD symptom scores on the ASRS.
The correlations were moderate and directionally consistent. SIRT-1 correlated with symptom severity at r = -0.430, Nrf-2 at r = -0.446, and HO-1 at r = -0.424.
- SIRT-1 and ASRS: Lower SIRT-1 aligned with higher symptom severity.
- Nrf-2 and ASRS: Lower Nrf-2 showed the strongest reported correlation among the three redox markers.
- HO-1 and ASRS: Lower HO-1 followed the same negative direction.
Correlation does not establish mechanism. It does show that the biomarker differences were not isolated from the clinical phenotype measured in the same participants.
ROC Results Suggested Moderate Biomarker Discrimination
The researchers also tested whether the markers could distinguish the ADHD and control groups using receiver operating characteristic analysis. This analysis estimates classification performance, not clinical readiness.
The three antioxidant-defense markers showed moderate discrimination: HO-1 AUC = 0.797, Nrf-2 AUC = 0.756, and SIRT-1 AUC = 0.753. An AUC of 0.5 means no discrimination, while 1.0 means perfect separation.
- Best single marker: HO-1 had the highest reported area under the curve.
- Clinical limit: Moderate AUC values are not enough to diagnose ADHD from blood testing.
- Research use: The markers may help future studies stratify oxidative-stress biology in adult ADHD.
For now, the biomarker profile is best read as a biological clue. ADHD remains a clinical diagnosis based on symptoms, impairment, developmental history, and differential diagnosis.
Cross-Sectional Blood Markers Need Replication in Larger ADHD Cohorts
The main limitation is design. A cross-sectional study cannot tell whether lower SIRT-1, Nrf-2, and HO-1 contribute to ADHD biology, reflect downstream stress exposure, or shift with treatment, sleep, diet, medication, or comorbid conditions.
The sample was also modest. A 120-person study can identify a signal, but biomarker claims need larger cohorts, medication subgroup analysis, longitudinal follow-up, and ideally independent replication.
- Medication context: Stimulant or non-stimulant treatment history can affect physiology and should be separated in future work.
- Comorbidity context: Anxiety, depression, sleep problems, and metabolic conditions may influence inflammatory and redox measures.
- Longitudinal context: Repeated measurements could test whether marker levels change with symptom improvement or clinical worsening.
The narrow interpretation is that adult ADHD in this cohort was associated with a lower serum SIRT-1/Nrf-2/HO-1 defense profile, while TNF-alpha did not differ. That gives researchers a testable biomarker pattern, not a blood test for ADHD.
Citation: DOI: 10.1007/s11011-026-01845-5. Gürbüzer et al. The SIRT-1/Nrf-2/HO-1 antioxidant defense axis in adult attention-deficit/hyperactivity disorder. Metabolic Brain Disease. 2026;41:85.
Study Design: Cross-sectional case-control biomarker study in adults with ADHD and matched healthy controls.
Sample Size: 60 adults with ADHD and 60 age- and sex-matched healthy controls.
Key Statistic: SIRT-1, Nrf-2, and HO-1 were lower in adults with ADHD, with all three group comparisons at p < 0.001 and ASRS correlations from r = -0.424 to r = -0.446.
Caveat: Cross-sectional blood-marker data cannot show whether the redox differences cause ADHD symptoms or result from other clinical and lifestyle factors.





