TL;DR: A 2026 study in Psychopharmacology found that healthy adults who used cannabis frequently had higher circulating THC markers after at least 12 hours of verified abstinence, but their cold-pressor pain threshold, pain tolerance, and pain ratings did not differ from occasional users.
Key Findings
- 75 cannabis users were tested: the sample included 38 occasional users and 37 frequent users, ages 21 to 55, after biochemically verified brief abstinence.
- Frequent use meant about 6 days weekly: frequent users reported 6.2 cannabis-use days/week, compared with 2.6 days/week in the occasional-use group.
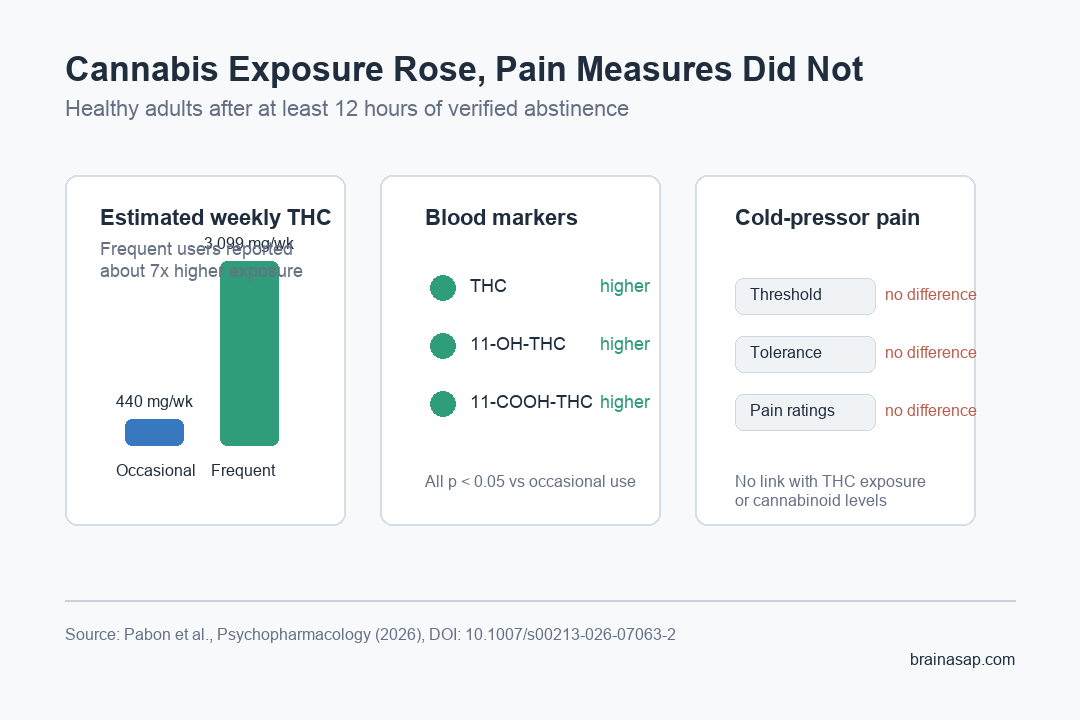
- Estimated THC exposure was much higher: weekly THC exposure averaged 3,099.3 mg in frequent users versus 439.7 mg in occasional users.
- THC biomarkers tracked use: frequent users had higher plasma THC, 11-OH-THC, and 11-COOH-THC, and weekly THC exposure correlated with THC and 11-COOH-THC levels.
- Pain outcomes stayed null: cold-pressor pain threshold, pain tolerance, and subjective pain ratings did not differ by cannabis-use frequency, weekly THC exposure, or circulating cannabinoid levels.
Source: Psychopharmacology (2026) | Pabon et al.
Cannabis is commonly used for pain, but the relationship between regular use, short-term abstinence, cannabinoid levels, and pain sensitivity is not straightforward. A person can have measurable THC metabolites in blood without showing a detectable change in an experimental pain task.
This study tested that distinction directly. Researchers brought healthy adults who reported past-month cannabis use into the lab after at least 12 hours of verified abstinence.
They measured circulating cannabinoids and used the Cold Pressor Test, a standard task in which participants keep a hand in cold water until pain threshold and tolerance are reached.
Frequent Cannabis Use Raised THC Biomarkers During Brief Abstinence
The use-pattern contrast was large. Frequent users reported cannabis use on 6.2 days per week, while occasional users reported 2.6 days per week.
That difference also showed up in estimated dose exposure. Frequent users averaged 3,099.3 mg of THC per week, compared with 439.7 mg per week in the occasional-use group.
- THC: the main intoxicating cannabis compound measured in plasma.
- 11-OH-THC: an active THC metabolite that can still reflect recent exposure.
- 11-COOH-THC: a non-intoxicating THC metabolite often used as a longer-lasting exposure marker.
Frequent users had significantly higher plasma levels of all 3 THC-related measures. The statistical tests were strongest for 11-COOH-THC, with p < 0.001, and also significant for THC and 11-OH-THC.
Cold-Pressor Pain Threshold and Tolerance Did Not Differ
The pain result went in the other direction: it was mostly absent. Pain threshold, pain tolerance, and subjective pain ratings did not significantly differ between frequent and occasional cannabis users.
Weekly THC exposure also did not predict the pain outcomes. In practical terms, the people with much higher estimated weekly THC intake and higher plasma THC markers did not show lower pain tolerance during this brief abstinence window.
The finding matters because cannabis withdrawal and pain sensitivity are often discussed together. This study does not show that cannabis has no role in pain biology, but it does argue against a simple short-abstinence hyperalgesia pattern in healthy adults.
Cannabinoid Levels Did Not Explain Pain Ratings
Researchers also tested whether measured cannabinoid levels mapped onto pain perception across the whole sample. They did not. Pain threshold, tolerance, and ratings were not associated with plasma phytocannabinoids or endocannabinoids.
That included the THC-related compounds as well as endogenous lipid signaling molecules involved in cannabinoid biology. The study measured anandamide (AEA), 2-AG, OEA, and PEA, but these values did not explain the pain task results.
- Exposure marker: weekly THC exposure was linked to plasma THC and 11-COOH-THC.
- Pain marker: the cold-pressor task did not shift with use frequency or THC exposure.
- Mechanism marker: measured cannabinoid and endocannabinoid levels did not account for pain ratings.
The cleanest interpretation is narrow: in this sample and time window, cannabis-use intensity showed up biologically but not behaviorally in acute cold pain perception.
Sex Differences Appeared in Endocannabinoid-Related Lipids
One secondary result involved sex differences. Females had higher AEA, OEA, and PEA concentrations than males, independent of cannabis-use pattern.
Those differences did not translate into detectable pain differences in this study. Still, they are useful because cannabinoid and endocannabinoid studies can miss sex-dependent biology when analyses treat the whole sample as one uniform group.
- AEA: an endocannabinoid often called anandamide.
- OEA and PEA: related fatty-acid ethanolamides that interact with pain, inflammation, and metabolic signaling pathways.
- Study implication: sex may shape circulating lipid-signaling profiles even when the behavioral pain task remains unchanged.
The Null Pain Result Has a Short-Abstinence Boundary
The main caveat is timing. Participants were abstinent for at least 12 hours, not for several days or weeks. Longer abstinence could produce different withdrawal, mood, sleep, or pain-sensitivity effects.
The sample was also healthy rather than a clinical pain population. People using cannabis for chronic pain may respond differently from healthy adults completing a laboratory cold-water task.
Several limits shape how far the result should travel:
- Brief abstinence: the study tested a short verified abstinence period, not sustained withdrawal.
- Healthy adults: participants were not selected for chronic pain or cannabis-use disorder treatment.
- Self-reported dose estimates: weekly THC exposure depended on reported frequency, amount, and product THC concentration.
- Experimental pain task: cold-pressor pain is controlled and useful, but it is not the same as everyday migraine, neuropathic pain, or musculoskeletal pain.
Practical takeaway: higher recent cannabis exposure can be visible in blood without producing measurable cold-pain hypersensitivity after brief abstinence. For pain questions, abstinence duration and clinical population probably matter as much as use frequency.
Citation: DOI: 10.1007/s00213-026-07063-2. Pabon et al. Cannabis use patterns and perception of acute pain during brief abstinence: sex-dependent associations with circulating cannabinoid levels. Psychopharmacology. 2026.
Study Design: Laboratory observational study of cannabis-use frequency, estimated THC exposure, blood cannabinoid measures, and cold-pressor pain outcomes during verified brief abstinence.
Sample Size: 75 healthy adults who reported past-month cannabis use; 38 occasional users and 37 frequent users.
Key Statistic: Frequent users averaged 3,099.3 mg weekly THC exposure versus 439.7 mg in occasional users, but pain threshold, tolerance, and ratings did not differ by use frequency or THC exposure.
Caveat: The abstinence period was short and the sample was healthy, so the null pain result should not be treated as a chronic-pain or long-withdrawal finding.





