
TL;DR: A 2026 randomized trial in PLOS One found that one week of Bhagavad Gita learning, alone or paired with yoga, was associated with lower Generalized Anxiety Disorder-7 (GAD-7) scores in Indian healthcare workers, with the strongest 45-day responder rate in the Gita-only group.
Key Findings
- 68 healthcare workers: Researchers randomized 17 participants each to yoga, Bhagavad Gita learning, combined yoga plus Gita learning, or usual care.
- One-week intervention: Yoga used 60-minute daily sessions, Gita learning used 60-minute daily teaching of Chapter 2, and the combined arm used 30 minutes of each.
- Immediate anxiety difference: Yoga plus Gita learning produced lower immediate post-intervention GAD-7 scores than usual care after multiplicity adjustment (p = 0.009).
- 45-day Gita difference: Gita learning alone produced lower delayed GAD-7 scores than usual care at 45 days (p = 0.047).
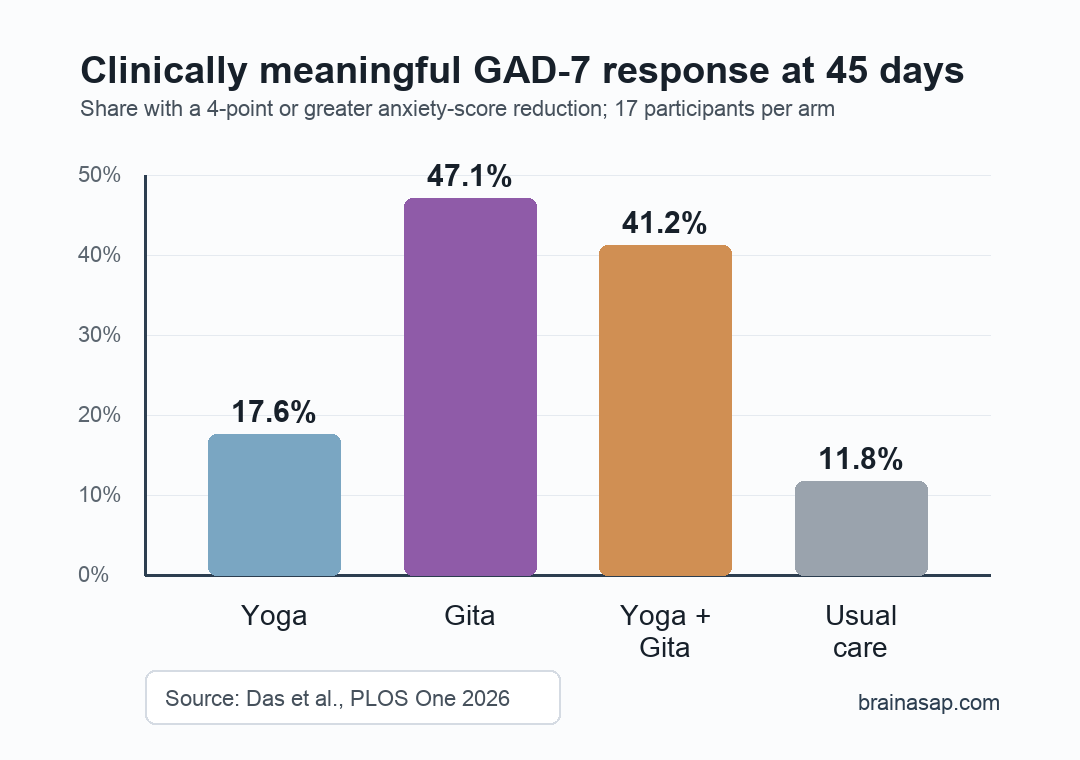
- Responder rates differed: A clinically meaningful 4-point GAD-7 reduction at 45 days occurred in 47.1% of the Gita group, 41.2% of the combined group, 17.6% of the yoga group, and 11.8% of controls.
Source: PLOS One (2026) | Das et al.
Healthcare Workers Were Randomized to Yoga, Gita Learning, Both, or Usual Care
Healthcare workers often carry pandemic-era stress while also facing stigma around formal mental-health support. This trial tested whether culturally familiar practices could lower anxiety symptoms in a setting where counseling and peer-support services had low uptake.
The trial enrolled 68 healthcare workers at a secondary hospital in India. Participants had no diagnosed pre-existing mental-health condition and were randomly assigned to one of four groups:
- Yoga: Daily 60-minute yoga sessions for one week.
- Gita learning: Daily 60-minute teaching sessions on Chapter 2 of the Bhagavad Gita for one week.
- Yoga plus Gita: Daily 30-minute yoga plus 30-minute Gita teaching sessions for one week.
- Control: Usual care without the structured intervention.
Anxiety symptoms were measured with the Generalized Anxiety Disorder-7 (GAD-7), a seven-item screening scale where higher scores indicate more anxiety symptoms. Researchers measured scores at baseline, immediately after the one-week intervention, and again 45 days later.
Gita Learning Had the Clearest 45-Day Anxiety Difference
At baseline, GAD-7 scores did not differ meaningfully across trial arms. That baseline balance made the later differences less likely to reflect one group simply starting with lower anxiety.
Median GAD-7 scores in the Gita group moved from 7 at baseline to 4 immediately after treatment and 3 at 45 days. The usual-care control group stayed near its starting level, with a median score of 7 at baseline, 6 immediately after, and 7 at 45 days.
The adjusted between-group comparison found that Gita learning differed from usual care at 45 days (p = 0.047). Yoga plus Gita differed from usual care immediately after the intervention (p = 0.009), but its 45-day comparison narrowly missed the same threshold after adjustment (p = 0.057).
Clinically Meaningful Response Was Highest in the Gita Group
The clearest reader-facing number is the share of participants who had a clinically meaningful GAD-7 reduction, defined in the paper as a drop of at least 4 points from baseline to the delayed follow-up.
Responder rates were uneven across groups:
- Gita learning: 8 of 17 participants responded, or 47.1%.
- Yoga plus Gita: 7 of 17 participants responded, or 41.2%.
- Yoga alone: 3 of 17 participants responded, or 17.6%.
- Usual care: 2 of 17 participants responded, or 11.8%.
In exploratory odds-ratio analysis, the odds of achieving that response were higher for Gita learning versus control (OR 6.67, 95% CI 1.15 to 38.60). The combined intervention also had a higher but less precise estimate (OR 5.25, 95% CI 0.90 to 30.62).
Those intervals are wide because each arm had only 17 people. The responder analysis is useful for understanding practical effect size, but it should not be read as definitive proof that one spiritual or movement practice is superior to another.
The Trial Tested a Cultural Access Problem, Not Only a Relaxation Technique
The study is also about acceptability. Researchers described earlier local experience in which only a small fraction of healthcare workers used counseling or peer-support services, partly because seeking formal mental-health help can carry stigma.
That context explains why the intervention used culturally familiar material rather than a generic stress-management lecture. In this trial, Bhagavad Gita learning functioned as structured cognitive and spiritual reframing, while yoga added a physical practice that is already common in many stress-reduction programs.
The intervention design had three practical features:
- Short duration: The active intervention lasted only one week, making it easier to imagine in a workplace setting than a long therapy course.
- Group-compatible format: Sessions could be delivered to staff as teaching or practice blocks rather than private clinical visits.
- Cultural fit: Nearly all participants were practicing Hindus, so the Gita arm matched the population more closely than it would in a religiously mixed or non-Hindu workforce.
Small Size and Expectancy Effects Limit the Claim
The evidence is narrow. This was a single-center trial with 68 total participants, and the sample was not broadly representative of all healthcare workers.
Participants knew which group they were in. That awareness could introduce expectancy or performance bias, especially in the spiritually based intervention arms.
Outcome assessors and data analysts were blinded, which helps. The lived experience of the intervention still could not be blinded.
Several other limits matter for interpretation:
- Religious generalizability: The findings may not apply to healthcare workers from other faith backgrounds or to workers who prefer secular support.
- Adherence measurement: Continued practice was measured with a simple yes/no question, not detailed practice logs.
- Comparator choice: Usual care does not control for extra attention, group contact, or instructor time.
Practical takeaway: the study supports culturally matched, low-stigma stress-support programs as a plausible workplace mental-health tool. It does not prove that Bhagavad Gita learning should replace counseling, medication, formal therapy, or broader staffing and workload reforms.
Citation: DOI: 10.1371/journal.pone.0347320. Das et al. The stress reduction potential of Bhagavad Gita and Yoga for healthcare workers during the COVID-19 pandemic: A randomized controlled trial. PLOS One. 2026;21(4):e0347320.
Study Design: Prospective, single-center, four-arm randomized controlled trial.
Sample Size: 68 healthcare workers, with 17 assigned to each group.
Key Statistic: Clinically meaningful 45-day GAD-7 response occurred in 47.1% of the Gita group and 41.2% of the combined group, compared with 11.8% of controls.
Caveat: Small single-center sample, unblinded participants, usual-care comparator, and limited generalizability beyond a mostly Hindu healthcare-worker sample.





