TL;DR: A 2026 review in Reviews in the Neurosciences argues that chemotherapy-induced peripheral neurotoxicity (CIPN), nerve injury from cancer treatment, can involve central nervous system changes that help explain chronic neuropathic pain and chemotherapy-related cognitive impairment.
Key Findings
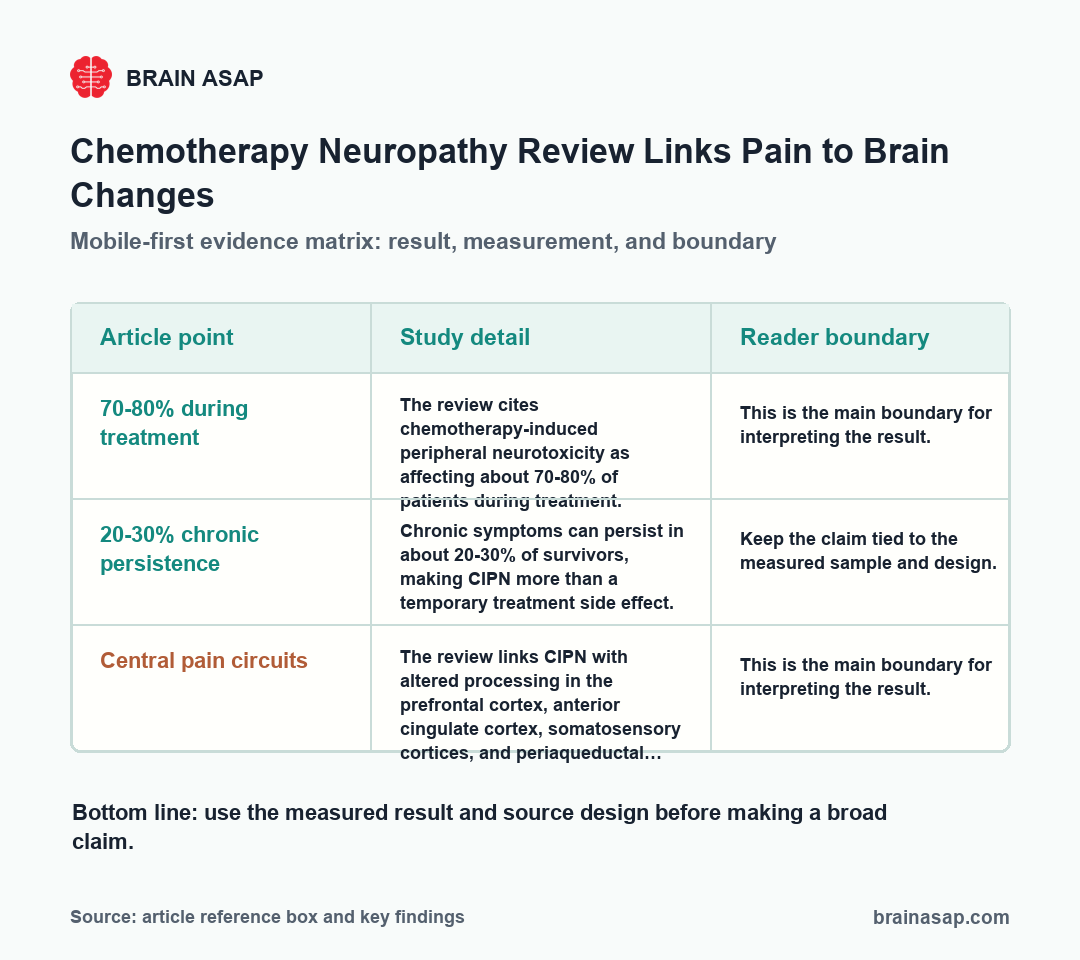
- 70-80% during treatment: The review cites chemotherapy-induced peripheral neurotoxicity as affecting about 70-80% of patients during treatment.
- 20-30% chronic persistence: Chronic symptoms can persist in about 20-30% of survivors, making CIPN more than a temporary treatment side effect.
- Central pain circuits: The review links CIPN with altered processing in the prefrontal cortex, anterior cingulate cortex, somatosensory cortices, and periaqueductal gray.
- Inflammation bridge: Peripheral nerve injury can promote cytokine dysregulation, microglial activation, and blood-brain barrier stress.
- Cognitive pathway: The review connects CIPN biology with hippocampal-dependent memory, synaptic plasticity, adult neurogenesis, and “chemobrain” symptoms.
Source: Reviews in the Neurosciences (2026) | Cherchi et al.
Chemotherapy-induced peripheral neurotoxicity is usually introduced as a peripheral nerve problem. Patients can develop numbness, tingling, burning pain, cold sensitivity, and altered sensation after drugs that injure sensory nerves.
The Cherchi review broadens that model. Peripheral nerve damage still comes first, but the long-term syndrome can also involve brain circuits that process pain, emotion, attention, and memory.
Chemotherapy Neuropathy Is Not Only a Peripheral Nerve Problem
CIPN deserves attention because cancer survival can leave patients with persistent nervous-system symptoms. The review cites a high treatment-period burden, with 70-80% of patients affected during chemotherapy and 20-30% of survivors reporting chronic symptoms.
Peripheral nerve injury remains the primary pathology. Chemotherapy can damage sensory neurons, disrupt axons, alter ion channels, and create abnormal pain input from the body to the spinal cord.
Chronic neuropathic pain is rarely just a one-way message from the injured nerve. Repeated pain input can change spinal and supraspinal processing, making the nervous system more responsive to signals that were previously tolerable.
That shift is central sensitization: pain-processing circuits become easier to activate. In CIPN, that means a chemotherapy-triggered injury can continue through altered central regulation even after the original treatment exposure has ended.
This can change how symptoms are interpreted. A survivor can have ongoing pain even when the original chemotherapy exposure is over, because the nervous system has learned a more reactive pain state.
Central Pain Regions Included PFC, ACC, Somatosensory Cortex, and PAG
The review emphasizes several brain regions involved in pain modulation.
The prefrontal cortex (PFC) helps with evaluation, control, and attention to pain. The anterior cingulate cortex (ACC) contributes to pain affect and conflict monitoring.
Somatosensory cortices map body sensation, while the periaqueductal gray (PAG) participates in descending pain control. Together, these regions help decide how pain is perceived, regulated, and linked to behavior.
- Sensory coding: Somatosensory cortex can change how abnormal peripheral input is mapped.
- Affective pain: ACC and insula-related networks can connect pain with distress and salience.
- Top-down control: PFC and PAG pathways can alter descending inhibition or facilitation of pain.
These brain-level changes do not mean the pain is imaginary. They mean chemotherapy injury can change the whole pain system, from peripheral nerves through central pain-control networks.
That distinction changes patient care. A purely peripheral model points mainly toward protecting nerves or quieting abnormal sensory input, while a peripheral-central model also asks how the brain is amplifying, interpreting, and regulating that input.
It also helps explain why symptom severity does not always map neatly onto visible nerve damage. Two people can have similar peripheral injury but different pain persistence if descending control, stress biology, sleep, mood, or inflammatory signaling differs.
Neuroinflammation Could Connect Nerve Injury to Chemobrain
The review also links CIPN with chemotherapy-related cognitive impairment, often called chemobrain. The proposed bridge is inflammation rather than a simple pain-only pathway.
Peripheral nerve injury can trigger cytokine dysregulation and microglial activation. Microglia are immune-like support cells in the central nervous system that can amplify inflammatory signaling when activated.
Researchers also discuss blood-brain barrier stress. A weaker barrier can make the brain more exposed to circulating inflammatory signals, which can affect synaptic plasticity and hippocampal-dependent memory.
Hippocampal dysfunction is especially relevant because the hippocampus supports learning and memory. If chemotherapy-related inflammation disrupts hippocampal plasticity or adult neurogenesis, cognitive symptoms and persistent pain may share part of the same biology.
The review does not treat chemobrain as a vague complaint. It places cognitive symptoms inside mechanisms that can be measured: inflammatory mediators, blood-brain barrier integrity, hippocampal plasticity, and neural circuits that support attention and memory.
That approach is useful because cancer survivors can describe pain, fatigue, memory lapses, and concentration problems together. A shared inflammatory and circuit-level framework can help researchers test whether those symptoms travel together biologically.
The review also makes the cognitive claim more specific than a general complaint of fogginess. It points to hippocampal memory, synaptic plasticity, and neurogenesis as candidate targets for future measurement.
Animal Models Help Trace the Peripheral-to-Central Cascade
Human CIPN studies are clinically important, but they cannot easily map every step from chemotherapy exposure to nerve injury to central circuit change. Animal models help because researchers can measure tissues, pathways, and timing more directly.
The review describes animal evidence for central nervous system engagement beyond peripheral pathology. That includes altered neurotransmission, neuroinflammation, and changes in brain regions involved in pain and cognition.
- Glutamate and GABA balance: Excitatory and inhibitory neurotransmission can shift in pain-processing pathways.
- Ion-channel changes: Voltage-gated channels can alter neuronal excitability after chemotherapy exposure.
- Microglial activation: Inflammatory glial responses can contribute to persistent pain and cognitive effects.
The evidence does not prove a single linear pathway for every patient. Different chemotherapy drugs, doses, cancer contexts, and individual vulnerabilities can create different mixtures of peripheral and central mechanisms.
Drug specificity is one reason future work needs treatment-specific grouping. Platinum agents, taxanes, vinca alkaloids, and other anticancer drugs can injure nerves through partly different mechanisms, so one CIPN pathway does not explain every survivor’s pain or cognition profile.
Timing is also important. Studies that measure only after chronic symptoms are established can miss the early sequence from nerve injury to inflammatory signaling to central sensitization.
Repeated assessment could separate early peripheral toxicity from later central amplification. That would help researchers identify when prevention, anti-inflammatory treatment, pain-modulation therapy, or cognitive support has the best chance to work.
Mechanism-Based CIPN Treatment Needs Brain Outcomes
Current CIPN treatment remains limited. The review notes that recommended options largely focus on symptomatic relief, with duloxetine often used for painful CIPN.
A central nervous system model changes what future studies should measure. Pain intensity is still important, but researchers also need cognition, mood, sleep, sensory processing, and biomarkers of neuroinflammation or barrier function.
That broader measurement approach could identify patient subgroups. A survivor whose symptoms are driven mainly by peripheral axon injury can need different treatment than someone with strong central sensitization, cognitive symptoms, and inflammatory changes.
The review also points toward combined endpoints. A trial could track pain ratings, quantitative sensory testing, cognitive tasks, sleep, mood, and inflammatory markers rather than treating each domain as a separate problem.
For patients, the immediate message is not that brain-targeted CIPN treatments are ready. The clearer point is that persistent chemotherapy neuropathy deserves a nervous-system-wide explanation when pain and cognitive symptoms continue after cancer treatment.
The cautious conclusion is direct: CIPN should not be reduced to damaged peripheral nerves alone. Persistent chemotherapy neuropathy may involve a coupled peripheral-central disorder, where pain and cognition are shaped by nerve injury, inflammation, and brain-network regulation.
Citation: DOI: 10.1515/revneuro-2025-0146. Cherchi et al, From peripheral neurotoxicity to central dysfunction: linking neuropathic pain and cognition in chemotherapy-induced peripheral neuropathy. Reviews in the Neurosciences. 2026.
Study Design: Narrative review synthesizing human and animal evidence on CIPN, pain pathways, and cognition.
Sample/Model: Chemotherapy-induced peripheral neurotoxicity literature across clinical patients and preclinical models.
Key Statistic: CIPN is framed as involving peripheral nerve injury plus central pain, inflammatory, and cognition-related mechanisms.
Caveat: Review evidence cannot define a single cause-effect sequence for all chemotherapy drugs or patient subgroups.