TL;DR: A 2026 systematic review and meta-analysis in European Journal of Psychotraumatology found that phase-based therapy was not clearly better than non-phase-based therapy for most complex PTSD outcomes, although multi-phase treatment had stronger PTSD effects and phase/exposure-based approaches improved affect dysregulation more.
Key Findings
- Sixteen randomized trials were included: Researchers reviewed psychological interventions for complex PTSD or PTSD with disturbances in self-organization symptoms.
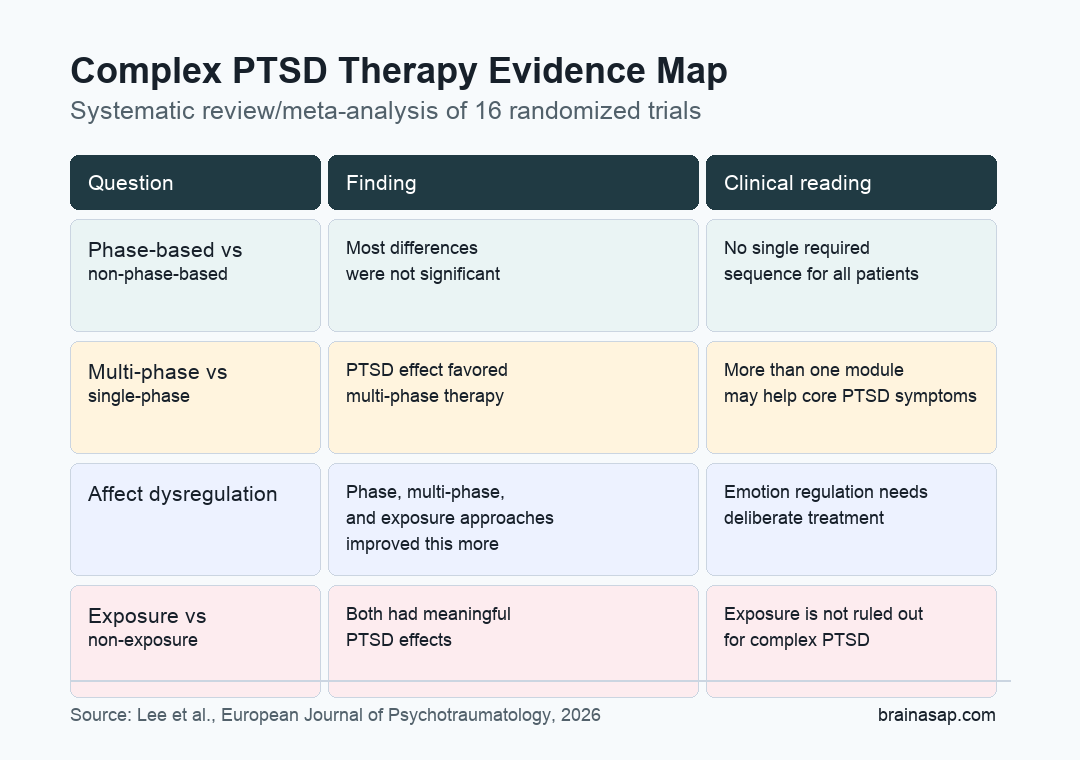
- Most subgroup differences were not significant: Phase-based therapy, non-phase-based therapy, exposure therapy, and non-exposure therapy often showed overlapping effects.
- Multi-phase therapy helped PTSD symptoms more: Against waitlist or treatment-as-usual controls, multi-phase interventions had a larger PTSD effect than single-phase interventions.
- Affect dysregulation showed a clearer treatment-sequencing pattern: Phase-based, multi-phase, and exposure interventions had larger effects on this emotion-regulation component of complex PTSD.
- The evidence base remains small: The review was limited by few eligible trials, single post-treatment time points, and heterogeneous outcome measures.
Source: European Journal of Psychotraumatology (2026) | Lee et al.
Complex PTSD Treatment Did Not Require One Universal Sequence
Complex post-traumatic stress disorder (CPTSD) includes the core PTSD symptoms of re-experiencing, avoidance, and persistent threat, plus disturbances in self-organization (DSO): affect dysregulation, negative self-concept, and relationship disturbance.
That broader symptom profile has created a practical treatment question. Should therapy begin with stabilization and skills work before trauma memory exposure, or can some patients move directly into trauma-focused treatment without a formal first phase?
Researchers reviewed randomized trials that could speak to that question. Their central result was restrained: across most outcomes, phase-based interventions were not clearly superior to non-phase-based interventions.
Treatment structure still mattered in some comparisons. The current trial evidence simply does not support a single mandatory sequence for every person with complex PTSD symptoms.
The Review Compared Phases, Modules, and Exposure
The researchers searched major medical, psychology, trauma, and South Korean databases on June 17, 2025. Eligible studies had to be randomized controlled trials of psychological interventions for people with clinically significant CPTSD symptoms or PTSD plus at least two DSO symptom clusters.
The review separated three treatment questions that are often blended together:
- Phase-based therapy: Treatment that placed stabilization first, followed by trauma-focused exposure or memory work.
- Multi-phase therapy: Treatment that included more than one phase, even if it did not follow the exact stabilization-before-exposure sequence.
- Exposure-based therapy: Treatment that included re-experiencing or reappraisal of traumatic memories, such as prolonged exposure or EMDR-style work.
The distinction is important because a therapy can be multi-module without being phase-based in the classic sense. A treatment can also include exposure without requiring a long stabilization period first.
Sixteen Trials Made It Through Screening
The search started with 1,642 records. After duplicate removal, title/abstract screening, and full-text review, 16 randomized trials met the inclusion criteria.
The included studies were clinically varied. Eleven were conducted in Europe, two in North America, and three in East Asia.
Some focused on childhood abuse survivors, intimate partner violence survivors, veterans, refugees, students, or people with broader complex trauma histories.
Researchers also had to work across different symptom measures. Six studies used the International Trauma Questionnaire (ITQ), which directly reflects ICD-11 CPTSD criteria.
Others used older or indirect measures, including the Structured Interview for Disorders of Extreme Stress or selected PTSD Checklist items.
That measurement spread is one reason the findings should be read as a careful evidence map rather than a final clinical rule.
Multi-Phase Therapy Had the Clearest PTSD Advantage
Against waitlist or treatment-as-usual controls, the pooled effect on PTSD symptoms was moderate to large. The overall PTSD estimate was Hedges’ g = -0.58, with a 95% confidence interval from -0.82 to -0.35.
The phase-based comparison leaned in favor of phase-based treatment, but the difference was not statistically significant. Phase-based interventions had an estimated PTSD effect of g = -0.94, while non-phase-based interventions had g = -0.50.
The clearest separation came from the number of treatment phases. Multi-phase interventions showed a significantly larger PTSD effect than single-phase interventions:
- Multi-phase interventions: g = -0.70, 95% CI -0.93 to -0.48.
- Single-phase interventions: g = -0.15, 95% CI -0.62 to 0.33.
- Between-group test: Q = 4.28, p = .04, favoring multi-phase treatment.
Affect Dysregulation Looked More Sensitive to Structure
The DSO-affect dysregulation finding is clinically important because it captures problems with intense emotion, emotional shutdown, and difficulty returning to baseline after distress. In CPTSD, affect dysregulation is not a side issue; it is part of the diagnostic pattern.
Here, structured approaches showed stronger results. Phase-based, multi-phase, and exposure interventions improved DSO-affect dysregulation more than their comparison groups.
That result fits a practical interpretation. Many patients may not need one fixed sequence to improve PTSD symptoms, but emotion-regulation symptoms may benefit from treatment designs that deliberately combine skills, trauma processing, and integration.
The review does not prove that stabilization must always come first. It suggests that affect regulation may need to be treated deliberately, especially when emotional dysregulation is one of the reasons trauma work becomes difficult.
Exposure Therapy Was Not Simply Too Risky
One concern in CPTSD treatment is that exposure to traumatic memories may overwhelm patients who have longstanding emotion-regulation problems or complex interpersonal trauma. The review did not support a simple avoid-exposure rule.
Exposure and non-exposure interventions both showed meaningful PTSD effects. In the waitlist/treatment-as-usual comparison, exposure interventions had g = -0.61, while non-exposure interventions had g = -0.54. The difference was not significant.
For clinicians and patients, the point is not that exposure is always needed. It is that exposure-based work cannot be dismissed as categorically inappropriate for complex PTSD based on the current randomized-trial evidence.
Several treatment decisions still belong at the individual level:
- Readiness: Whether the person can tolerate trauma-memory work without destabilizing daily functioning.
- Symptom target: Whether PTSD re-experiencing, affect dysregulation, relationship symptoms, or negative self-concept is the immediate clinical priority.
- Comorbidity: Whether substance use, suicidality, dissociation, depression, or personality-disorder symptoms require extra monitoring.
- Access: Whether the available treatment is structured, evidence-informed, and delivered by clinicians trained for trauma complexity.
The review’s limitations are not minor. Only 16 trials were eligible, and the subgroup analyses sometimes rested on much smaller sets.
Several outcomes could be examined only at the immediate post-treatment time point because follow-up timing differed across studies.
Outcome heterogeneity also limits interpretation. A trial using the ITQ is not identical to a trial that approximates DSO symptoms with older or indirect measures.
This makes pooled estimates helpful for orientation, but weaker as a basis for rigid treatment rules.
The safest clinical reading is direct: non-phase-based and non-exposure-based therapies can work for many CPTSD-relevant outcomes, while multi-phase or exposure-inclusive designs may be especially helpful for PTSD symptoms and affect dysregulation in some contexts.
Future trials need larger samples, clearer ICD-11 CPTSD measurement, longer follow-up, and head-to-head designs that compare treatment sequences without mixing too many therapy ingredients at once.
Citation: DOI: 10.1080/20008066.2026.2644112. Lee et al. Phase-based versus non-phase-based psychological interventions for complex PTSD: a systematic review and meta-analysis. European Journal of Psychotraumatology. 2026;17:2644112.
Study Design: Systematic review and meta-analysis of randomized controlled trials comparing psychological intervention components for complex PTSD symptoms.
Sample Size: Sixteen randomized trials from an initial search set of 1,642 records.
Key Statistic: Multi-phase therapy had a larger PTSD effect than single-phase therapy in waitlist/treatment-as-usual comparisons (Hedges’ g -0.70 vs -0.15; Q = 4.28, p = .04).
Caveat: Few eligible trials, heterogeneous outcome measures, and inconsistent follow-up timing limit the precision of subgroup conclusions.