TL;DR: A 2026 review and activation-likelihood estimation study in European Journal of Pain found that the dorsolateral prefrontal cortex (dlPFC), a frontal control region, was repeatedly engaged in acute pain, chronic pain, and placebo analgesia, mainly across Brodmann areas 8, 9, and 46.
Key Findings
- 138 studies included: The review screened 4810 deduplicated records and extracted dlPFC activation or connectivity coordinates from 138 eligible human neuroimaging studies.
- More than 4000 participants: Combined samples included acute pain (n = 814), chronic pain (n = 2467), placebo analgesia (n = 791), conditioned pain modulation (n = 184), and offset analgesia (n = 47).
- BA 8, 9, and 46: Acute pain, chronic pain, and placebo analgesia showed convergent dlPFC clusters mainly in Brodmann areas 8, 9, and 46.
- No simple laterality: Acute pain, chronic pain, placebo analgesia, and miscellaneous pain modulation showed bilateral dlPFC involvement rather than a single left- or right-sided pattern.
- Targeting implication: The findings refine candidate dlPFC subregions for neuromodulation research, but they do not prove that stimulating one spot will relieve pain.
Source: European Journal of Pain (2026) | Crawford et al.
The dorsolateral prefrontal cortex (dlPFC) is often discussed as if it were one pain-control site. This review treated it as a larger cortical territory with many subregions.
The practical mapping question was whether human imaging coordinates for dlPFC involvement in pain or analgesia converge on the same parts of that broad prefrontal region.
138 Neuroimaging Studies Mapped dlPFC Pain Coordinates
The review searched PubMed, Web of Science, and Scopus, with the final search run on May 5, 2025. After duplicate removal, 4810 records were screened for eligibility.
Eligible studies had to involve human functional brain imaging, report whole-brain analyses, and provide standard-space activation maxima in the dlPFC. Region-of-interest-only studies and papers without usable coordinates were excluded.
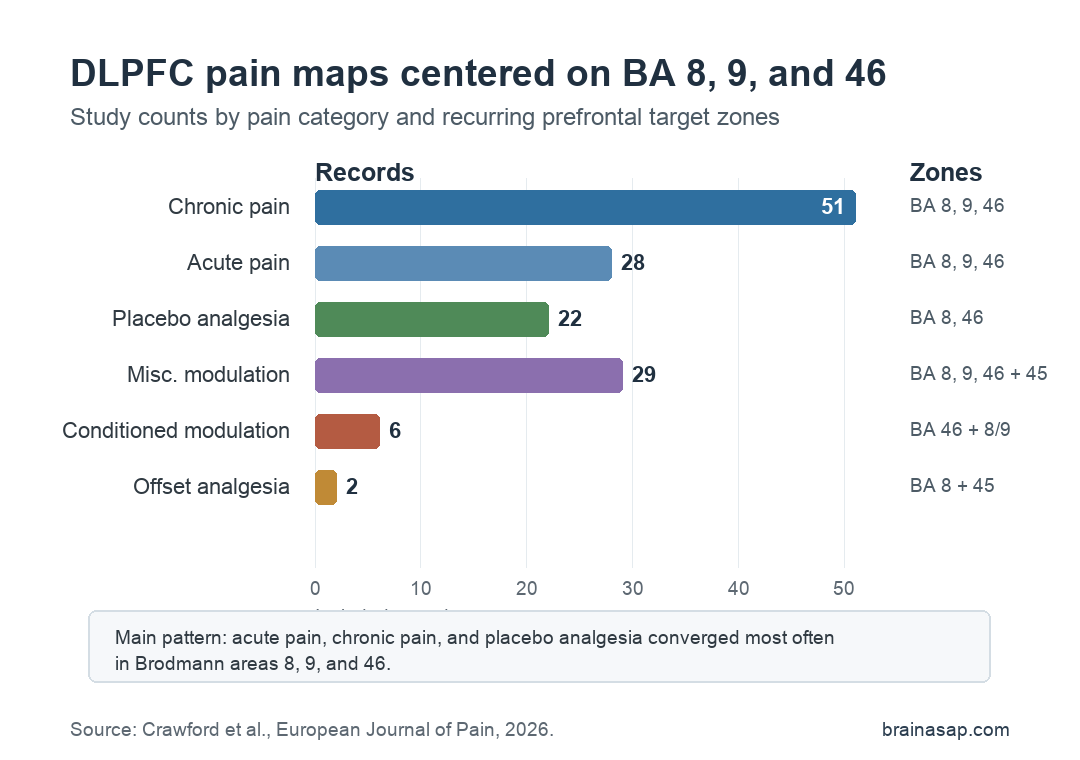
- Acute pain: 28 records with a combined sample of 814 participants.
- Chronic pain: 51 records with a combined sample of 2467 participants.
- Placebo analgesia: 22 records with a combined sample of 791 participants.
- Other modulation: Conditioned pain modulation, offset analgesia, and miscellaneous pain-modulation studies were analyzed separately.
The main method was activation likelihood estimation (ALE), a coordinate-based meta-analysis approach that identifies where reported brain-imaging peaks converge across studies.
They then overlaid those ALE maps onto an extended Human Connectome Project parcellation of dlPFC. This let them ask whether pain-related peaks clustered in Brodmann areas 8, 9, 46, or nearby inferior frontal regions.
Acute Pain, Chronic Pain, and Placebo Analgesia Shared BA 8-9-46 Clusters
The broad finding was anatomical consistency. Acute pain in pain-free participants, chronic pain states, and placebo analgesia all showed dlPFC engagement primarily in Brodmann areas 8, 9, and 46.
For acute pain, 25 of 28 studies, or 89%, reported signal increases. The most frequent locations included left and right 8C, BA46, and 9-46d.
Chronic pain looked more mixed. Fewer chronic-pain studies reported dlPFC increases than acute-pain studies did, and chronic pain included both increases and decreases across similar broad regions.
- Acute pain: ALE clusters appeared bilaterally and mainly occupied BA 8, BA 9, and BA 46.
- Chronic pain: ALE clusters also appeared in both hemispheres, again centered on BA 8, BA 9, and BA 46.
- Placebo analgesia: Bilateral clusters occupied BA 8 and BA 46, resembling the acute and chronic pain maps more than a separate analgesia-only zone.
This overlap supports a specific interpretation: the dlPFC is not only a reaction to pain intensity. It also appears in the cognitive-control and expectation systems that can change pain experience.
Conditioned and Offset Analgesia Had Smaller Evidence Bases
The more specialized pain-modulation categories were much smaller. Conditioned pain modulation included 6 studies, and offset analgesia included only 2 studies.
Conditioned pain modulation is the phenomenon where one painful stimulus can reduce the perceived intensity of another. Offset analgesia is the disproportionate pain relief that can follow a small drop in noxious stimulus intensity.
- Conditioned pain modulation: Signal changes most often involved BA 46, with ALE clusters involving BA 46, BA 8, BA 44, and BA 9.
- Offset analgesia: Only two studies were available, with clusters involving left BA 8 and BA 45.
- Miscellaneous modulation: Expectancy, emotional modulation, attention, hypnosis, music, exercise, and non-invasive brain stimulation studies were grouped together and showed broader dlPFC scatter.
Because the specialized categories were small, they are less stable than the acute pain, chronic pain, and placebo analgesia findings. The review is strongest when it identifies repeated BA 8-9-46 involvement, not when it separates every analgesic mechanism.
DLPFC Pain Maps May Improve Neuromodulation Targets
The clinical motivation is neuromodulation. Non-invasive brain stimulation studies often target the dlPFC for pain, but the dlPFC spans many parcels, and a broad label can hide meaningful anatomical differences.
The review suggests that stimulation research should pay closer attention to the specific dlPFC subregions most often implicated in pain perception and modulation. BA 8, BA 9, and BA 46 are the recurring zones, not the entire frontal lobe.
The limitations are important. The search strategy required dlPFC to be a core concept in the title, abstract, or keywords, so the review may miss pain-imaging studies that reported dlPFC findings without foregrounding that region.
- Mixed modalities: The analysis combined task activation and resting functional connectivity studies.
- Coordinate dependence: Studies without usable standard-space maxima were excluded.
- Chronic-pain bias: Chronic-pain studies had higher risk concerns around randomization and adverse-event reporting.
The main takeaway for pain treatment is cautious. The review narrows likely dlPFC pain-relevant territory, but trials still need to test whether targeting those subregions changes symptoms in specific pain conditions.
Citation: DOI: 10.1002/ejp.70318. Crawford et al. The Human Dorsolateral Prefrontal Cortex in Pain and Pain Modulation: A Review and Activation-Likelihood Estimation Approach. European Journal of Pain. 2026;30:e70318.
Study Design: PRISMA-aligned review with coordinate-based activation likelihood estimation and dlPFC parcel frequency analysis.
Sample Size: 138 human neuroimaging studies, including more than 4000 participants across pain and pain-modulation categories.
Key Statistic: Acute pain, chronic pain, and placebo analgesia converged mainly in dlPFC Brodmann areas 8, 9, and 46.
Caveat: The analysis maps imaging-coordinate convergence and does not prove that stimulation of one dlPFC parcel will relieve clinical pain.