TL;DR: A 2026 study in Journal of Pain Research found that spinal cord stimulation and dorsal root entry zone lesioning reduced pain for selected patients with refractory postherpetic neuralgia, but the evidence came from a 10-patient single-center series.
Key Findings
- 10 refractory PHN patients: The retrospective series included 6 men and 4 women treated between 2011 and 2023, with postherpetic neuralgia symptoms lasting 7 to 192 months.
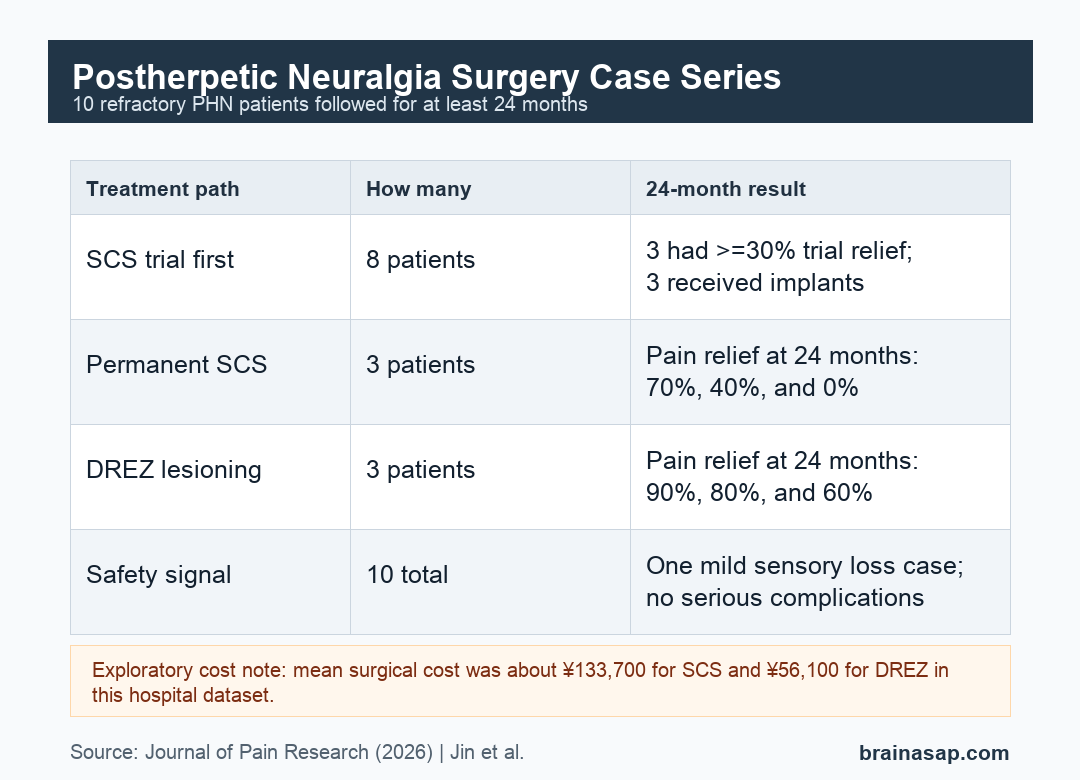
- 8 SCS trials: 8 patients tried spinal cord stimulation, and 3 reached the trial threshold of at least 30% pain reduction before permanent implantation.
- 3 permanent SCS implants: At 24 months, the implanted patients had pain relief rates of 70%, 40%, and 0%, showing that early benefit did not always persist.
- 3 DREZ procedures: 3 patients underwent dorsal root entry zone lesioning, with 24-month pain relief rates of 90%, 80%, and 60%.
- No serious complications: 1 DREZ patient developed mild segmental sensory loss without functional limitation, and no motor weakness, wound infection, or cerebrospinal fluid leak was reported.
Source: Journal of Pain Research (2026) | Jin et al.
Postherpetic Neuralgia Cases Had Severe Long-Lasting Pain
Postherpetic neuralgia is chronic nerve pain that can persist after a shingles rash heals. In this series, patients had pain for a mean of 53.2 months, and one patient had symptoms for 192 months.
The group was small but clinically severe. 9 of the 10 patients started with a Numeric Rating Scale pain score of 10 out of 10, and the remaining patient started at 8 out of 10.
Researchers described thoracic dermatomes as the main pain distribution. The distribution is clinically relevant because postherpetic neuralgia often tracks damaged sensory roots, dorsal root ganglia, and dorsal horn pathways rather than a diffuse whole-body pain pattern.
All patients had already tried multiple conventional treatments before surgery, including oral drugs such as anticonvulsants or antidepressants and interventional treatments such as nerve blocks, epidural injections, radiofrequency ablation, or intrathecal therapy.
Spinal Cord Stimulation Helped Only Some Trial Responders
Spinal cord stimulation (SCS) uses an epidural electrode to modulate pain signaling through the dorsal columns. In this study, SCS was treated as a reversible first surgical step rather than an automatic permanent implant.
8 patients entered an SCS trial. The trial counted as positive only if pain fell by at least 30% on the Numeric Rating Scale and the improvement lasted for at least 48 hours with better daily activity.
The SCS pathway separated patients quickly:
- Trial success: 3 of 8 trial patients reached the response threshold and received permanent implants.
- Trial failure: 5 of 8 did not get enough relief, so the temporary electrodes were removed.
- Long-term durability: among the 3 implanted patients, 24-month pain relief was 70%, 40%, and 0%.
Mean pain scores among the implanted patients improved from NRS 10.0 before surgery to 4.0 at 1 month, then drifted to 6.3 at 24 months. Mean Pain Disability Index scores decreased from 52.3 to 37.0 at the final follow-up.
The most practical message is that SCS can work, but trial response and sustained response are not the same thing. A patient with an implant initially improved, lost benefit within 2 months, and requested device removal.
DREZ Lesioning Produced Larger Pain Relief in 3 Patients
Dorsal root entry zone (DREZ) lesioning is a more invasive operation that targets hyperactive pain pathways where sensory roots enter the spinal cord. It is not reversible in the way an SCS system is.
3 patients underwent DREZ lesioning. 1 had failed an SCS trial first, and 2 declined SCS and received DREZ as their primary surgical procedure.
At 24 months, the DREZ group showed larger pain reductions than the SCS implant group in this small dataset:
- Patient 8: pain decreased from NRS 10 at baseline to 1 at final follow-up, a 90% pain relief rate.
- Patient 9: pain decreased from NRS 10 to 4, a 60% pain relief rate.
- Patient 10: pain decreased from NRS 10 to 2, an 80% pain relief rate.
Functional disability also improved. Mean Pain Disability Index scores in the DREZ group decreased from 59.3 to 17.3, suggesting that pain reduction translated into daily-function gains for these patients.
The researchers also reported visible nerve-root changes during surgery. In the DREZ cases, atrophic dorsal roots lined up with the dermatomes identified before surgery, supporting the idea that the operation was targeting damaged pain pathways rather than an unrelated spinal level.
Safety and Cost Results Favored Different Tradeoffs
The safety findings were reassuring but limited by the sample size. No device-related infections, hardware malfunctions, permanent neurological deficits, motor weakness, cerebrospinal fluid leaks, or wound infections were reported.
1 DREZ patient developed mild segmental sensory loss at the treated levels without functional impairment. That fits the tradeoff clinicians worry about: DREZ can directly interrupt pain pathways, but it is a lesioning procedure near sensory spinal cord structures.
The cost comparison also pointed in two directions:
- SCS reversibility: SCS was less destructive and could be tested before permanent implantation.
- SCS expense: mean total surgical cost was about Y133,700, largely because of the implantable pulse generator.
- DREZ expense: mean total surgical cost was about Y56,100 in this hospital dataset.
- Local economics: the cost figures were reported in Chinese Yuan at 2023 price levels, so they may not transfer directly to other health systems.
Hospital stay went in the same general direction, with a mean of 18.4 days for SCS and 13.7 days for DREZ lesioning.
Patient Selection Remains the Main Clinical Question
This study does not establish that DREZ is broadly superior to SCS. The groups were tiny, treatment was not randomized, and the more invasive procedure may have been chosen for different anatomy, symptoms, or patient preference.
Still, the case series gives a useful clinical frame. SCS may be most reasonable when pain pathways can still be modulated through the dorsal columns and a trial produces clear coverage and relief.
DREZ lesioning may fit a different patient profile, especially when there is failed SCS, visible dorsal-root injury, dorsal horn signal change on imaging, or a strongly segmental pain pattern suggesting more fixed spinal-cord-level pathology.
Important limits should stay front and center:
- Small sample: only 10 patients were included, with 3 permanent SCS implants and 3 DREZ procedures.
- Single center: surgical expertise, patient selection, and cost structures may differ elsewhere.
- Retrospective design: the analysis can describe outcomes but cannot prove the best treatment sequence.
- Incomplete predictors: imaging and neurophysiological markers were not analyzed systematically enough to create firm selection rules.
For patients with refractory postherpetic neuralgia, the result supports a careful neurosurgical discussion rather than a simple ranking of procedures. The strongest next step would be prospective multicenter work that links pain distribution, spinal imaging, neurophysiology, and long-term quality-of-life outcomes.
Citation: DOI: 10.2147/JPR.S583921. Jin et al. Spinal Cord Stimulation and DREZ Lesioning for Refractory Postherpetic Neuralgia: An Exploratory Case Series. Journal of Pain Research. 2026;19:583921.
Study Design: Retrospective single-center exploratory case series of neurosurgical treatment for refractory postherpetic neuralgia.
Sample Size: 10 patients with refractory postherpetic neuralgia; 8 underwent SCS trials, 3 received permanent SCS implants, and 3 underwent DREZ lesioning.
Key Statistic: At 24 months, DREZ-treated patients had pain relief rates of 90%, 80%, and 60%; permanent SCS implant patients had pain relief rates of 70%, 40%, and 0%.
Caveat: The sample was very small and nonrandomized, so the findings are best read as patient-selection clues rather than comparative proof.





