TL;DR: A 2026 medRxiv preprint found that nonverbal Theory of Mind (ToM), the ability to infer another person’s beliefs or perspective, varied in 44 adults with post-stroke aphasia and was more closely tied to vascular brain-health markers than to aphasia severity.
Key Findings
- Study group: 44 adults with aphasia after mostly left-hemisphere stroke completed 2 low-language false-belief tasks.
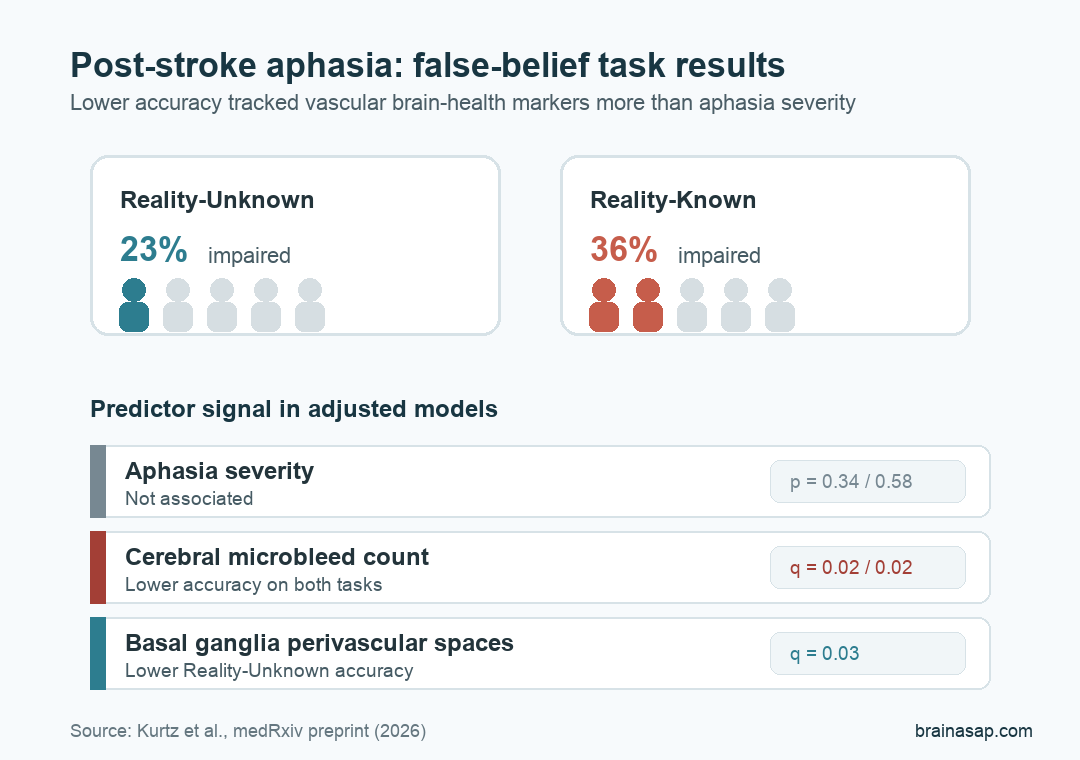
- Task result: Reduced performance appeared in 23% on the Reality-Unknown task and 36% on the Reality-Known task.
- Aphasia severity: Western Aphasia Battery-Revised Aphasia Quotient scores were not associated with task accuracy.
- Vascular marker: Higher cerebral microbleed count was associated with lower accuracy on both tasks after correction.
- Caution: This is a preprint and the MRI-marker analyses used smaller subsets, mostly 28 to 32 participants.
Source: medRxiv preprint (2026) | Kurtz et al.
Social cognition after stroke is often harder to measure than language, movement, or memory.
A person may score poorly on a social-reasoning task because language demands are too high, because the task requires inhibition, or because broader brain injury has affected the networks needed to follow another person’s perspective.
This preprint tested that problem in post-stroke aphasia. Researchers used 2 nonverbal false-belief tasks, meaning tasks built to test belief reasoning with minimal spoken or written language demands.
44 Adults With Aphasia Completed 2 False-Belief Tasks
The study included 44 adults with aphasia. Mean age was 59.1 years, and the average Western Aphasia Battery-Revised Aphasia Quotient was 81.8, with a wide range from 31.5 to 100.
The central question was not whether aphasia itself makes social cognition impossible. It was whether task performance after stroke tracks aphasia severity or whether it also reflects vascular brain-health markers such as microbleeds, white-matter changes, lacunes, and enlarged perivascular spaces.
- Theory of Mind: The ability to infer another person’s beliefs, intentions, or perspective.
- False-belief task: A task where one person in a scene holds a belief that differs from reality.
- Reality-Unknown task: A lower-inhibition version where participants did not directly know the object’s first location.
- Reality-Known task: A higher-inhibition version where participants had to suppress their own knowledge of reality.
Cerebral small vessel disease (CSVD) was the vascular-brain-health frame. Researchers measured markers including white matter hyperintensities, cerebral microbleeds, lacunes, and enlarged perivascular spaces.
Reduced Performance Was More Common on the Higher-Inhibition Task
Performance was mixed, not uniformly normal and not uniformly impaired. On the Reality-Unknown task, 10 of 44 participants, or 23%, were classified as impaired. On the Reality-Known task, 16 of 44 participants, or 36%, were classified as impaired.
The difference fits the task design. The Reality-Known version asks people to hold reality in mind while also using another person’s mistaken belief.
That adds self-perspective inhibition, which may be difficult after stroke even when the task avoids heavy language demands.
Important boundary: these tasks do not prove that everyday social understanding is impaired in every person with aphasia. They show that a meaningful subset had difficulty on structured belief-reasoning tasks even when language demands were reduced.
Aphasia Severity Did Not Explain False-Belief Accuracy
The cleanest negative result was about aphasia severity. Western Aphasia Battery-Revised Aphasia Quotient scores were not significantly associated with accuracy on either task: p = 0.34 for Reality-Unknown and p = 0.58 for Reality-Known.
A low-language task can still be misread as a language result if the analysis stops at aphasia. In this sample, the severity of aphasia did not explain who performed worse.
- Language measure: WAB-R Aphasia Quotient, a standard aphasia-severity score.
- Lesion measure: Lesion volume was included in adjusted models when available.
- Age adjustment: The aphasia-severity result remained nonsignificant after accounting for age and lesion volume.
Practical interpretation: a person with aphasia can have social-reasoning difficulty that is not simply a direct function of language severity. Assessment may need to test social cognition directly instead of assuming language scores capture the whole problem.
Cerebral Microbleed Count Tracked Lower Task Accuracy
The stronger association came from vascular brain-health markers. Cerebral microbleed count was associated with lower accuracy on both false-belief tasks after false-discovery-rate correction: q = 0.02 for Reality-Unknown and q = 0.02 for Reality-Known.
Basal ganglia enlarged perivascular spaces were also linked to lower Reality-Unknown accuracy after correction, with q = 0.03. The Reality-Known association was weaker after correction, with q = 0.09.
- Microbleeds: Small MRI-visible traces of prior bleeding from fragile small vessels.
- Enlarged perivascular spaces: Fluid-filled spaces around small brain vessels, often read as one marker of small-vessel burden.
- White matter hyperintensities: MRI-visible white-matter changes; these were not associated with task accuracy in this analysis.
- Lacunes: Small prior infarcts; lacune count had an unadjusted Reality-Unknown association that did not survive correction.
These results support a broader interpretation: social-reasoning task performance after stroke may reflect distributed vascular brain health, not only the aphasia diagnosis or the size of the main lesion.
The Preprint Should Be Read as a Small, Focused Signal
The finding narrows a common clinical assumption. If a person with aphasia struggles on a social-cognition task, the explanation may not be “language impairment made the task too hard.” Vascular brain-health markers may also shape the outcome.
The limits are equally important. The manuscript is a preprint, so it has not completed peer review.
MRI-marker sample sizes were smaller than the full behavioral sample: several CSVD analyses used 28 to 32 participants.
- Best use: Treat the study as evidence that social cognition after aphasia deserves direct measurement.
- Do not overread: Do not use the findings as a clinical diagnostic rule for individual patients.
- Next test: Replicate the pattern in larger stroke cohorts with everyday social-function outcomes.
The clinical point is straightforward: low-language social-cognition tests can reveal more than aphasia severity. In this preprint, poorer nonverbal belief reasoning was most consistently tied to cerebral microbleed count, suggesting that vascular brain health may matter for social recovery after stroke.
Citation: DOI: 10.64898/2026.04.14.26350532. Kurtz et al. Mental-state reasoning or downstream vascular burden? Theory of Mind task performance in post-stroke aphasia. medRxiv. 2026.
Study Design: Preprint analysis of nonverbal false-belief task performance and cerebral small vessel disease markers after post-stroke aphasia.
Sample Size: 44 adults with aphasia completed the behavioral tasks; MRI-marker analyses used smaller subsets.
Key Statistic: Impaired performance was classified in 23% on Reality-Unknown and 36% on Reality-Known; cerebral microbleed count remained associated with lower accuracy on both tasks after correction.
Caveat: The study is a preprint and should be read as an early finding, not a clinical rule.





