TL;DR: A 2026 study in Biological Psychiatry: Global Open Science found that systemic low-frequency oscillation (sLFO), a slow whole-body physiology readout usually treated as functional MRI noise, tracked nicotine dependence, cue-induced craving, abstinence, and stimulant-related task performance across four fMRI cohorts.
Key Findings
- The study analyzed four fMRI cohorts: Researchers examined a 64-person cigarette cue-reactivity group, a chronic nicotine-use comparison group, 462 Human Connectome Project controls, and a 58-person randomized psychostimulant cohort.
- sLFO means systemic low-frequency oscillation: It is a slow blood-flow, respiration, and vascular timing pattern in functional magnetic resonance imaging (fMRI) data that is often removed as noise.
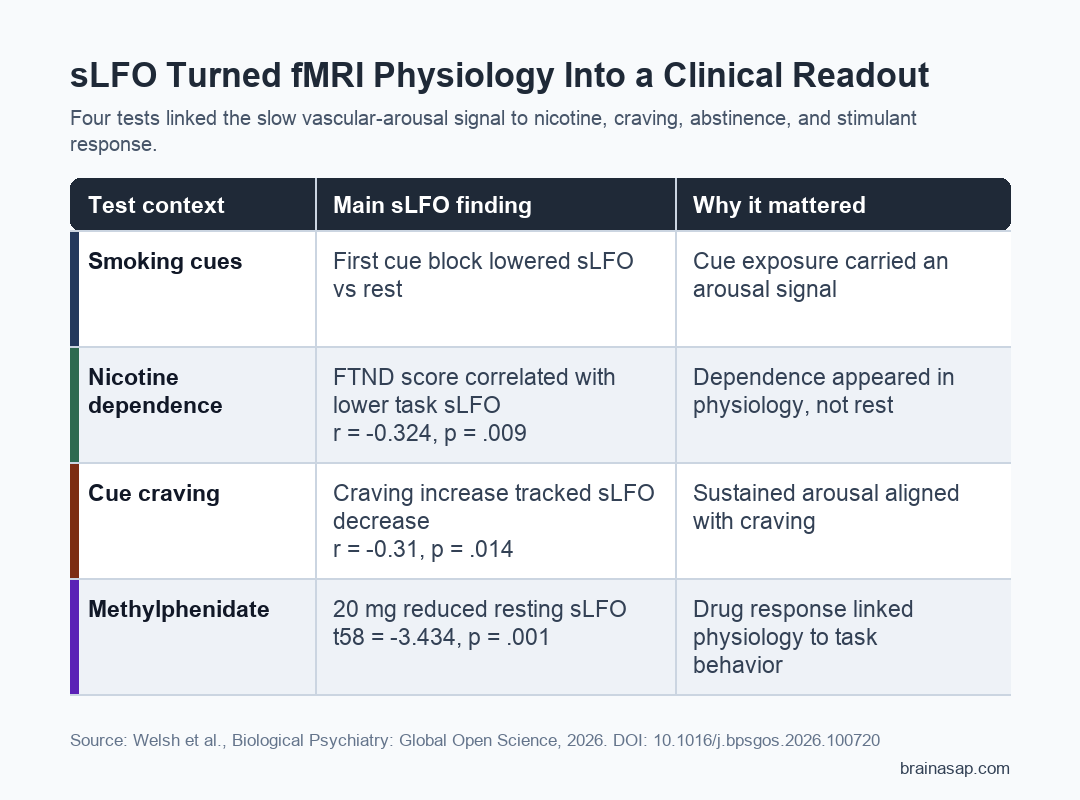
- Nicotine dependence tracked lower sLFO during smoking cues: In the cue-reactivity group, higher Fagerstrom Test for Nicotine Dependence scores correlated with lower task-average sLFO (r = -0.324, p = .009).
- Craving rose when sLFO fell across the cue task: Greater cue-induced craving was linked to a larger decrease in brainwide sLFO across the task (r = -0.31, p = .014).
- sLFO is not a standalone addiction biomarker: Results came from secondary analyses and small-to-moderate cohorts, so sLFO is better viewed as a reusable physiology layer inside existing fMRI data.
Source: Welsh et al. Biological Psychiatry: Global Open Science. 2026.
Functional magnetic resonance imaging, or fMRI, is usually used to study brain activity through blood oxygen level-dependent patterns. The same scan also carries physiology from breathing, blood flow, vascular tone, and arousal.
Many pipelines treat those slower physiology traces as nuisance variation. Researchers tested whether one of them, the systemic low-frequency oscillation (sLFO), had clinical information instead of just scanner noise.
The study’s practical claim is simple: a pattern removed from fMRI data may also describe the body’s arousal state. For nicotine use, craving, abstinence, and stimulant response, that physiology may be part of the clinically relevant picture.
sLFO Captured Slow Physiology Inside fMRI Data
sLFO refers to slow oscillations around 0.009 to 0.15 Hz that move through the brain with vascular timing delays.
The measure is influenced by blood flow, respiration, vasomotion, and autonomic arousal rather than a single local brain circuit.
The researchers used Regressor Interpolation at Progressive Time Delays, or RIPTiDe, to extract the pattern from standard fMRI scans.
That method estimates how the slow oscillation arrives across different voxels and produces both brainwide and voxelwise sLFO measures.
The study separated four related questions:
- Smoking cues: whether cigarette images changed sLFO in 64 people who smoked cigarettes.
- Nicotine abstinence: whether sLFO differed between smoking satiety and about 48 hours of abstinence in a chronic nicotine-use cohort.
- Scan-order control: whether repeated scanning alone shifted sLFO in 462 healthy Human Connectome Project participants.
- Psychostimulant challenge: whether nicotine or 20 mg methylphenidate altered sLFO and task performance in 58 healthy controls.
This design mattered because it avoided making one narrow cue-reactivity result carry the entire argument. Researchers asked whether the same physiology readout moved across cue exposure, withdrawal, stimulant administration, and cognitive performance.
Smoking Cues Lowered sLFO Early in the Task
In the cigarette cue-reactivity cohort, scan block had a significant effect on brainwide sLFO (F5,63 = 11.32, p < .001). The first smoking-cue block showed lower sLFO than rest and lower sLFO than later cue blocks.
The authors interpret lower sLFO as a marker of higher physiological arousal, consistent with prior work linking sLFO reductions to changes in heart rate variability, respiration, pupil diameter, and wake-sleep transitions.
That cue finding did not replace ordinary brain activation results. Smoking images still activated regions including medial prefrontal cortex, posterior cingulate cortex, precuneus, and angular gyrus, and the activation maps were highly similar with or without sLFO removal (spatial overlap r = 0.81).
In practical terms, sLFO and neural cue-reactivity maps appeared to describe different parts of the task. One captured broad physiology and arousal; the other captured task-related brain activation.
Nicotine Dependence and Craving Tracked the Physiology Readout
The clinical associations were the strongest reason to keep the readout visible. During the cue task, people with higher Fagerstrom Test for Nicotine Dependence scores had lower average sLFO (r = -0.324, p = .009).
At rest, that relationship was absent. Resting sLFO did not correlate with nicotine dependence in the cue-reactivity cohort or in the chronic nicotine-use cohort, which suggests the cue context mattered.
Craving showed a related dynamic pattern:
- Cue-induced craving: measured as the change in Questionnaire of Smoking Urges score from before to after the scan.
- sLFO change: measured as the difference between the last and first cue blocks.
- Main association: larger craving increases were linked to larger sLFO decreases across the cue task (r = -0.31, p = .014).
The association remained after controlling for sLFO during the first cue block (r = -0.26, p = .04).
That does not prove craving is caused by the physiology readout, but it supports the idea that sustained arousal during cue exposure adds information beyond brain activation maps alone.
Abstinence and Methylphenidate Shifted sLFO in Opposite Contexts
The chronic nicotine-use cohort added a withdrawal comparison. In a subset of 65 people who smoked cigarettes, brainwide sLFO was lower during nicotine satiety than after about 48 hours of abstinence (t64 = -4.51, p < .001).
Abstinent nicotine users also showed higher sLFO than healthy controls, including voxelwise increases in posterior cingulate cortex.
This result fits the authors’ interpretation that sLFO reflects an arousal-linked physiological state rather than only a trait difference between groups.
The stimulant cohort tested the same idea pharmacologically. Relative to placebo, acute nicotine did not change resting sLFO.
By contrast, 20 mg methylphenidate significantly decreased brainwide resting sLFO (t58 = -3.434, p = .001), with voxelwise decreases around regions including medial primary motor cortex, precuneus, and cuneus.
During the Multi-Source Interference Task, methylphenidate-related sLFO changes also tracked behavior:
- Reaction time: sLFO change correlated with faster responses in congruent and incongruent conditions (r = 0.38 and r = 0.39).
- Accuracy: sLFO change correlated with accuracy differences in both task conditions (r = -0.60 and r = -0.60).
- Nicotine challenge: acute nicotine did not track reaction time but was associated with accuracy changes.
The Finding Reframes Some fMRI “Noise”
The study does not say that every physiology artifact should be treated as a biomarker.
It argues for a more careful split: remove sLFO when the goal is a cleaner neural activation estimate, but also analyze it when arousal, substance use, medication, sleep, or autonomic physiology may be clinically relevant.
That distinction is important for psychiatry. Many psychiatric and substance-use studies already have archived fMRI data.
If sLFO can be extracted from those datasets, it may add a low-cost physiology layer without new scanning.
The limits are still real:
- Secondary analysis: the cohorts were assembled from existing studies with different aims and task designs.
- Sample sizes varied: the main nicotine cue cohort had 64 participants, and the drug challenge cohort had 58.
- Clinical specificity is unknown: sLFO may reflect arousal broadly, not a nicotine-specific or diagnosis-specific process.
- Prediction was not the main endpoint: the paper linked sLFO to clinical and behavioral variables but did not validate a diagnostic tool.
The practical takeaway is narrower and stronger. Some physiology removed from fMRI is not meaningless.
In this study, sLFO acted like a measurable arousal-related physiology readout that helped explain nicotine dependence, cue-induced craving, abstinence, stimulant effects, and task performance.
Citation: DOI: 10.1016/j.bpsgos.2026.100720. Study et al. Functional Magnetic Resonance Imaging Signal Typically Viewed as Noise Has Clinical Relevance in Psychiatry. Biological Psychiatry: Global Open Science. 2026.
Study Design: Secondary analysis of four independent fMRI cohorts testing systemic low-frequency oscillation during smoking cues, nicotine abstinence, scan-order control, and acute psychostimulant administration.
Sample Size: 64 people in the cigarette cue-reactivity cohort; 97 nicotine users and 34 controls in the chronic nicotine-use cohort; 462 Human Connectome Project controls; and 58 healthy controls in the acute psychostimulant cohort.
Key Statistic: In the cue-reactivity cohort, task-average sLFO was negatively associated with nicotine dependence (r = -0.324, p = .009), and cue-related sLFO decrease was associated with cue-induced craving (r = -0.31, p = .014).
Caveat: The findings show clinically meaningful physiology inside fMRI data, but they do not validate sLFO as a standalone diagnostic or treatment-selection biomarker.