TL;DR: A 2026 randomized controlled study in Pakistan Journal of Pharmaceutical Sciences found that adding 20 Hz repetitive transcranial magnetic stimulation (rTMS) to risperidone was linked with lower cognitive-factor and aggression scores after 4 weeks in schizophrenia patients.
Key Findings
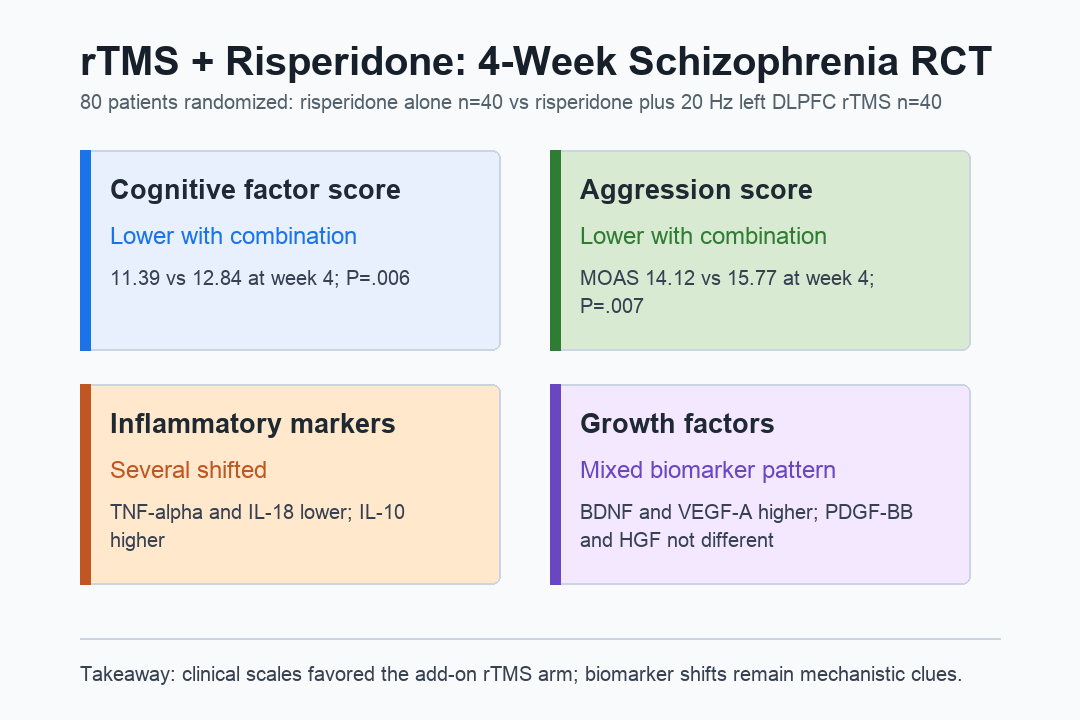
- Schizophrenia trial sample: The single-center trial randomized 80 patients, with 40 assigned to risperidone alone and 40 to risperidone plus rTMS.
- 4-week course: The add-on arm received 20 Hz rTMS over the left dorsolateral prefrontal cortex 5 days per week.
- Cognitive-factor score: Week-4 PANSS cognitive-factor scores were 11.39 with combination therapy versus 12.84 with risperidone alone.
- Aggression score: Week-4 Modified Overt Aggression Scale scores were 14.12 versus 15.77, favoring the combination arm.
- Serum markers: Several inflammatory and neurotrophic markers shifted, but PDGF-BB and HGF did not differ between groups.
Source: Pakistan Journal of Pharmaceutical Sciences (2026) | Zhou et al.
Schizophrenia cognition and aggression are difficult treatment targets. Risperidone can reduce positive symptoms, but cognition, impulse control, and behavioral dysregulation often remain clinically important.
This trial tested whether adding rTMS to risperidone changed those dimensions over a short 4-week treatment window.
rTMS Was Added to Risperidone for 4 Weeks
The study enrolled 80 adults with schizophrenia between February 2023 and February 2024. Participants were randomized into 2 equal groups after eligibility screening and sealed-envelope assignment.
Both groups received risperidone. The dose started at 1 mg/day and was titrated to a 4-6 mg/day maintenance range based on clinical response and tolerability.
The comparison therefore tested add-on stimulation rather than replacing antipsychotic medication.
The combination arm also received 20 Hz rTMS targeting the left dorsolateral prefrontal cortex, a prefrontal region often linked with executive control and working memory.
- Stimulation target: Left dorsolateral prefrontal cortex (DLPFC).
- Session pattern: 20-minute sessions, once daily, 5 times per week.
- Course length: 4 weeks of add-on stimulation.
- Intensity: 100% of cortical motor threshold.
No participants dropped out during treatment, so both groups contributed 40 patients to the week-4 comparisons. The report did not describe a sham stimulation arm.
PANSS Cognitive-Factor Scores Favored Add-On rTMS
Cognition was assessed with the cognitive-factor items from the Positive and Negative Syndrome Scale (PANSS). These items covered abstract thinking, spontaneity and fluency in conversation, and stereotyped thinking.
Baseline cognitive-factor scores were similar: 15.62 in the risperidone group and 15.71 in the combination group. After 4 weeks, the scores were 12.84 and 11.39, respectively, with P=.006.
- Direction: Both groups improved, but the combination group ended with the lower cognitive-factor score.
- Scale boundary: The measure used three PANSS negative-symptom items, not a full neuropsychological test battery.
- Timing: The week-4 finding does not show whether cognitive gains lasted after treatment ended.
The result supports add-on rTMS as a candidate strategy for schizophrenia-related cognitive symptoms, but it needs replication with broader cognitive testing.
Aggression Scores Also Improved More With Combination Treatment
Aggressive behavior was measured with the Modified Overt Aggression Scale (MOAS), a weighted scale covering verbal aggression, aggression toward property, self-directed aggression, and aggression toward other people.
Baseline MOAS scores were nearly identical: 23.76 in the risperidone group and 23.72 in the combination group. At week 4, the scores were 15.77 and 14.12, with P=.007.
- Behavioral endpoint: The week-4 MOAS score favored add-on rTMS.
- Clinical context: MOAS scores above 15 can indicate a level of aggression needing urgent management.
- Interpretation limit: The study did not isolate whether cognition, impulse control, symptom severity, or ward care drove the aggression change.
The aggression result is clinically relevant because it targets a practical safety dimension, not only a symptom-rating endpoint.
Inflammatory and Neurotrophic Markers Shifted Unevenly
The serum panel included tumor necrosis factor alpha (TNF-alpha), interleukins, brain-derived neurotrophic factor (BDNF), vascular endothelial growth factor A (VEGF-A), and other growth factors.
After treatment, the combination arm had lower TNF-alpha and IL-18, higher IL-10, higher BDNF, and higher VEGF-A than the risperidone-only arm. IL-8 and FGF-2 also differed between groups.
- Inflammation pattern: TNF-alpha was 11.25 versus 12.76 pg/mL, and IL-18 was 4.20 versus 5.39 pg/mL.
- Neurotrophic pattern: BDNF was 14.39 versus 13.14 pg/mL, and VEGF-A was 235.36 versus 220.72 pg/mL.
- Null markers: PDGF-BB and HGF showed no statistically significant post-treatment group differences.
These blood markers can help frame mechanism questions, but they do not prove that inflammation or neurotrophic signaling caused the clinical score changes.
Single-Center Design Keeps the Claim Narrow
The study has useful strengths: randomized assignment, equal group sizes, complete 4-week follow-up, and defined stimulation parameters. The design also has limits that matter for clinical interpretation.
It was a single-center study with 80 participants, short follow-up, and no separate sham rTMS control. The cognitive endpoint was a PANSS factor score rather than a detailed cognition battery.
- No sham arm: Expectation and care-contact effects cannot be fully separated from stimulation effects.
- Short window: A 4-week course is not enough to establish durable cognitive or behavioral benefit.
- Serum caveat: Peripheral biomarkers are indirect and can be influenced by medication, stress, inflammation, and sampling conditions.
- Next test: Larger sham-controlled trials should track cognition, aggression, symptoms, adverse events, and serum markers together.
For now, the measured clinical scales favored risperidone plus rTMS after 4 weeks, while the serum data remain supportive but not decisive.
Citation: DOI: 10.36721/PJPS.2026.39.5.15520.1. Zhou S, Tu H, Lin J. Effects of repetitive transcranial magnetic stimulation combined with risperidone on improving cognitive function and aggressive behavior in patients with schizophrenia and its effects on serum indicators. Pakistan Journal of Pharmaceutical Sciences. 2026;39(5):1452-1459.
Study Design: Single-center randomized controlled study comparing risperidone alone with risperidone plus rTMS.
Sample Size: 80 schizophrenia patients, with 40 assigned to each treatment group.
Key Statistic: Week-4 cognitive-factor scores were 11.39 with combination therapy versus 12.84 with risperidone alone, and MOAS scores were 14.12 versus 15.77.
Caveat: The trial lasted 4 weeks, used one center, and did not include a sham rTMS arm or full cognitive testing battery.