TL;DR: A 2026 systematic review and meta-analysis in International Journal of Obesity found that glucagon-like peptide-1 receptor agonists, metabolic drugs that extend a satiety and glucose-control hormone pathway, reduced body weight mainly through fat loss while lean-mass reductions were generally modest.
Key Findings
- 36 studies reviewed: Researchers included 36 studies in the qualitative review and 24 studies in the quantitative meta-analysis.
- Three time points tested: The meta-analysis pooled outcomes at 3, 6, and 12 months to compare body weight, BMI, waist circumference, fat mass, visceral fat, and lean mass.
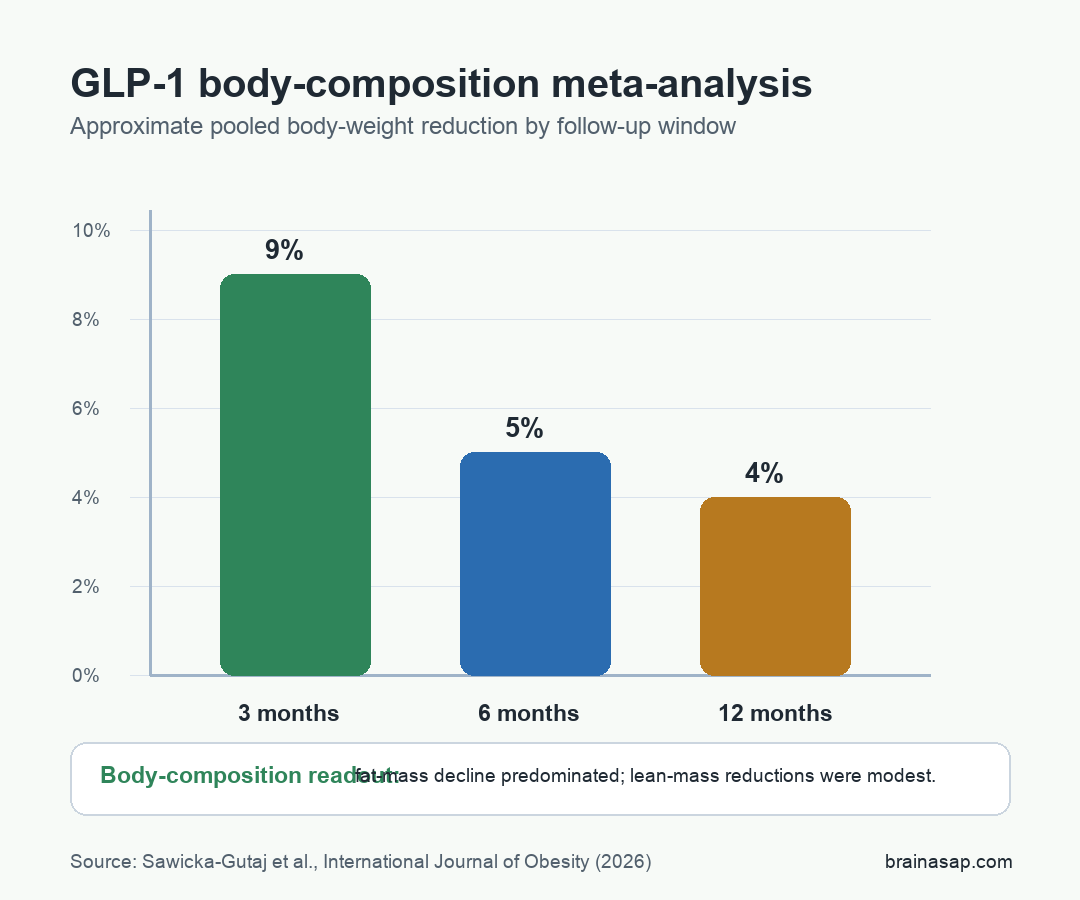
- About 9% at 3 months: Mean body weight decreased by approximately 9% at 3 months, with marked reductions in fat mass and visceral adipose tissue.
- About 5% at 6 months: Weight reduction averaged about 5% at 6 months, while semaglutide, liraglutide, and exenatide showed broadly comparable effects in the pooled analysis.
- About 4% at 12 months: Weight loss persisted around 4% at 12 months, with variability across agents and studies.
Source: International Journal of Obesity (2026) | Sawicka-Gutaj et al.
GLP-1 receptor agonists have changed obesity medicine because they do more than lower a number on a scale. The more practical question is what kind of tissue changes when weight falls.
This review focused on that question. It summarized how GLP-1 receptor agonists and dual GLP-1/GIP agonists affected body weight and body composition in adults with overweight or obesity, with or without type 2 diabetes.
GLP-1 Weight Loss Was Mostly a Fat-Mass Result
GLP-1-based treatment produced clinically meaningful weight loss, and the weight loss was driven mainly by reduced fat mass rather than large lean-mass depletion.
That distinction changes the clinical interpretation. Weight loss is not automatically healthy tissue loss.
A treatment that reduces total weight by stripping away muscle would be a different clinical problem from a treatment that mainly reduces excess adiposity.
The review described several body-composition outcomes that moved together:
- Body weight: GLP-1 receptor agonist treatment reduced weight across the pooled time points.
- BMI: Body mass index fell alongside body weight, as expected for a weight-loss intervention.
- Waist circumference: Central body-size measures decreased, supporting an abdominal-fat interpretation.
- Fat mass and visceral fat: The strongest tissue-level pattern was a reduction in fat stores, including visceral adipose tissue.
Lean body mass still needs attention. Any meaningful weight-loss treatment can reduce some lean mass, especially without resistance training, adequate protein intake, or careful follow-up.
The review’s broad conclusion was that lean-mass losses were modest relative to fat-mass losses.
Three-Month GLP-1 Results Showed the Steepest Early Change
The 3-month analysis produced the largest early change. Across included studies, mean body weight decreased by approximately 9%, accompanied by marked reductions in fat mass and visceral adipose tissue.
That early pattern fits how appetite and intake change when GLP-1 signaling is pharmacologically extended. These drugs increase satiety, slow gastric emptying, and reduce overall caloric intake, so the first months can show a steep drop before the trajectory slows.
The body-composition part is the more clinically relevant layer. Early weight loss can look impressive, but clinicians and patients still need to know whether the change is mostly fat, water, lean tissue, or a mixture.
In this review, the strongest early tissue result was fat reduction. That supports the phrase quality weight loss, meaning weight loss that preferentially reduces fat stores while limiting avoidable muscle loss.
Six- and Twelve-Month Findings Supported Ongoing Fat Reduction
At 6 months, average weight reduction was about 5% in the pooled analysis. Semaglutide, liraglutide, and exenatide showed broadly comparable effects at that point, while lean mass remained largely preserved.
At 12 months, weight loss persisted around 4%, although the review noted variability between agents and studies. Liraglutide was especially variable in the longer follow-up comparisons.
The time pattern should not be read as a universal patient trajectory. Meta-analyses blend different trials, populations, doses, diabetes status, and adherence patterns.
Still, the pooled result gives a practical scan of what the literature has been showing:
- Early reduction: The first months often show the fastest drop in body weight and fat mass.
- Longer follow-up: Weight loss can persist, but the pooled percentage changes become smaller and more variable.
- Body composition: Across time points, fat-mass decline remained more prominent than lean-mass decline.
Lean-Mass Preservation Still Depends on Nutrition and Exercise
The phrase relative preservation of lean tissue should not be mistaken for a guarantee. Lean mass can decline during weight loss, and the risk becomes more important in older adults, people with frailty, and anyone losing weight quickly.
The review explicitly pointed toward individualized treatment strategies, nutrition, and exercise interventions. That is not a decorative caveat. It is the practical route for turning pharmacologic weight loss into healthier body-composition change.
Three clinical details shape the interpretation:
- Resistance training: Muscle-loading exercise helps protect or rebuild lean tissue during weight loss.
- Protein adequacy: Appetite reduction can make it harder to meet protein needs unless diet is planned deliberately.
- Patient risk: Older age, low baseline muscle mass, chronic illness, and rapid dose escalation can change the risk-benefit balance.
The review did not test one standardized exercise or nutrition program across all included studies. It therefore supports the need for muscle-aware care, not a one-size-fits-all prescription.
GLP-1 Body-Composition Evidence Remained Heterogeneous
The most defensible conclusion is that GLP-1 receptor agonists reduce weight in a way that usually looks fat-dominant. The studies still differed by drug, dose, patient group, and follow-up period.
Systematic reviews help organize a scattered evidence base. They are also limited by the studies they inherit.
The included trials varied by agent, duration, diabetes status, body-composition method, and whether lifestyle support was built into the intervention.
Across the published evidence base, GLP-1 treatment can produce meaningful fat loss with modest lean-mass loss, but the healthiest version of that outcome still requires monitoring, nutrition, and exercise rather than medication alone.
That is the difference between a scale-centered result and a body-composition result. The scale says weight changed. This review suggests the more important tissue target was fat.
Citation: DOI: 10.1038/s41366-026-02088-1. Sawicka-Gutaj et al. GLP-1 agonists and changes in body mass and composition in adults with overweight or obesity with or without type 2 diabetes mellitus: a systematic review and meta-analysis. International Journal of Obesity. 2026.
Study Design: Systematic review and random-effects meta-analysis of GLP-1 receptor agonist and dual GLP-1/GIP agonist studies.
Sample Size: 36 studies in qualitative synthesis; 24 studies in quantitative meta-analysis.
Key Statistic: Approximate mean body-weight reductions were 9% at 3 months, 5% at 6 months, and 4% at 12 months, with fat-mass decline predominating.
Caveat: Study designs, agents, doses, durations, diabetes status, and body-composition methods varied, so patient-level muscle preservation still requires individualized monitoring.