TL;DR: A 2026 randomized single-blind trial in BMC Psychiatry found that a one-day lithium carbonate loading dose plus quetiapine reduced acute manic symptoms in bipolar I disorder more than standard slow-titration lithium plus quetiapine over 14 days.
Key Findings
- 60 inpatients randomized: Adults with bipolar I disorder in acute mania, all meeting DSM-5 criteria and scoring at least 20 on the Young Mania Rating Scale (YMRS), were assigned in equal blocks to a lithium loading-dose arm or a standard titration arm. Every patient also received quetiapine.
- Loading dose was 20 mg/kg on day one: The loading arm received lithium carbonate at 20 mg/kg up to 1,800 mg on day 1, then standard maintenance from day 2 onward. The standard arm started at 300 mg/day and stepped up in 300 mg increments every 2 to 3 days until reaching 900 to 1,200 mg/day.
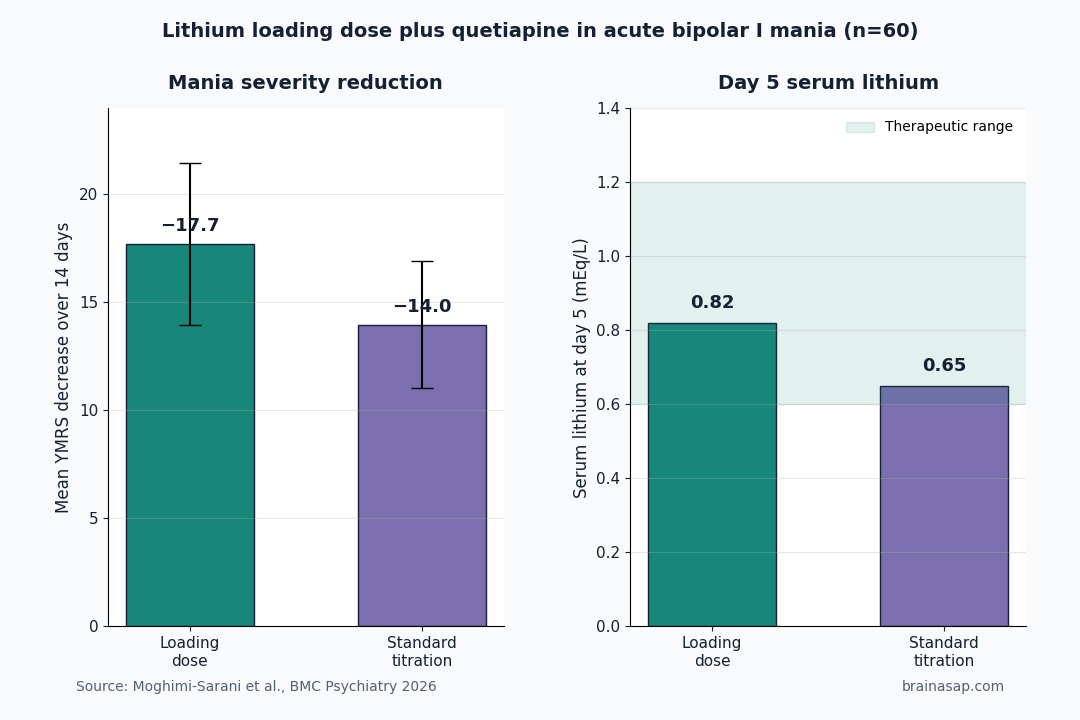
- Mania scores fell faster with loading: By day 14, the loading group had a mean YMRS decrease of −17.70 points compared with −13.96 in the standard group, a difference of about 3.7 points favoring loading (p < 0.001).
- Therapeutic lithium levels arrived sooner: Serum lithium in the loading group reached 0.82 mEq/L by day 5 compared with 0.65 mEq/L in the standard group, putting the loading arm inside the 0.6 to 1.2 mEq/L therapeutic range earlier in the admission.
- Both arms improved on quetiapine plus lithium: YMRS scores declined significantly in both groups across days 3, 7, and 14, so the comparison is between a faster-acting protocol and a slower one rather than between a working treatment and a failure.
Source: BMC Psychiatry (2026) | Moghimi-Sarani et al.
Acute mania is a psychiatric emergency. Untreated, it brings elevated mood, hyperactivity, impulsive risk-taking, sleep loss, and sometimes psychotic symptoms.
The longer mania lasts, the more functional and social damage it can do. The standard pharmacological approach combines a mood stabilizer with an antipsychotic, but the mood stabilizer side has a timing problem.
Lithium Works, But Slowly — And That Is the Problem
Lithium carbonate has been a first-line mood stabilizer for decades. It reduces relapse risk in bipolar disorder and lowers suicide risk over the long term.
Its acute anti-manic effect builds up over days, not hours, because the drug needs to reach a therapeutic serum concentration of about 0.6 to 1.2 mEq/L before the manic state begins to break.
Standard lithium dosing starts low and titrates up over days or weeks, partly out of caution about the drug’s narrow therapeutic window and risk of toxicity.
That caution is reasonable for long-term outpatient care. In an inpatient unit where someone is acutely manic, the same caution may extend the stay and prolong symptom exposure.
Quetiapine, an atypical antipsychotic, fills the early gap. It acts within hours rather than days, sedates, and reduces agitation.
The combination of quetiapine plus lithium is common practice. The question this Iranian trial asked is narrower: within that combination, can a one-day lithium loading dose shorten the time to lithium’s full contribution?
60 Inpatients, Block-Randomized, Same Quetiapine Backbone
Researchers at Shiraz University of Medical Sciences enrolled 60 adult inpatients in acute manic phase of bipolar I disorder. Inclusion required DSM-5 bipolar I diagnosis and a baseline YMRS score of at least 20, putting every participant into at least moderate mania.
Patients were block-randomized to two groups:
- Loading-dose lithium: A single weight-based dose of 20 mg/kg lithium carbonate on day 1, capped at 1,800 mg total, then standard maintenance dosing from day 2 forward.
- Standard-titration lithium: Started at 300 mg/day, increased in 300 mg increments every 2 to 3 days until reaching the conventional acute target of 900 to 1,200 mg/day.
- Shared quetiapine: Both arms started quetiapine at 100 mg/day split twice daily, then titrated up to a 400 to 800 mg/day target based on clinical response and tolerability.
The Young Mania Rating Scale, an 11-item clinician-rated scale of manic severity that scores irritability, sleep, language, content of thought, and several other domains, was the primary outcome. It was measured at baseline and on days 3, 7, and 14.
The Loading Arm Cleared More Mania Severity
Both groups improved over the 14-day window, which is expected given that both received an effective antipsychotic alongside lithium. The relevant question was how much each lithium protocol added to that improvement.
The loading group dropped a mean of 17.70 points (SD 3.76) on the YMRS from baseline. The standard group dropped 13.96 points (SD 2.94).
The between-group difference was statistically significant at p < 0.001. A 3-to-4 point YMRS difference in the moderate-to-severe range corresponds to a noticeable change in observed behavior, sleep, and engagement.
Serum lithium curves explain part of the gap. By day 5, the loading group’s mean lithium level was 0.82 mEq/L, sitting inside the therapeutic range.
The standard group sat at 0.65 mEq/L, just barely above the lower bound of therapeutic, and reached the trial’s higher levels later in the 14-day window.
Loading-Dose Lithium Is an Inpatient-Only Protocol With Tight Monitoring
This protocol is most relevant to inpatient settings where rapid manic-symptom control matters and where serum lithium levels can be monitored daily. The loading approach trades a slower titration period for higher day-1 exposure that needs careful follow-up.
- Time-to-therapeutic window: Loading shortened the time to therapeutic serum lithium by several days, which is the most direct lever a clinician has to shorten a manic admission.
- Combination context: Both arms received quetiapine, so the trial tested loading dose lithium as an addition to an antipsychotic, not loading dose lithium alone.
- Monitoring need: A 20 mg/kg day-1 dose requires close serum and clinical monitoring, especially for renal function, hydration, thyroid status, and signs of early lithium toxicity (tremor, gastrointestinal symptoms, confusion). The protocol works in a hospital with daily labs, not in an outpatient setting.
The size of the benefit is modest in absolute terms. A 3.7-point YMRS advantage is clinically real but not transformative.
That edge becomes meaningful in a patient population whose hospital days, suicide risk, and family burden all scale with how long the manic episode lasts.
Small Single-Center Sample and Single-Blind Design Limit Confidence
The trial has real constraints that should shape interpretation before any practice change:
- Single-center, single-country: 60 patients at one Iranian psychiatric hospital is not a global sample. Genetic, ethnic, and metabolic differences could affect lithium pharmacokinetics across populations.
- Single-blind: Patients were blinded but clinicians administering the dose and rating the YMRS were not. Rater blinding matters because YMRS scoring involves clinical judgment.
- 14-day window: The trial measured acute mania reduction over 14 days. It does not show whether loading-dose patients had different relapse rates, side effects, or adherence over the following 6 months.
- Safety reporting: Adverse events including renal, thyroid, and gastrointestinal effects need full reporting in the published trial, especially because higher day-1 exposure is the entire intervention.
None of these are reasons to dismiss the finding. They are reasons to wait for replication in a larger, ideally multi-center, double-blind trial before treating loading-dose lithium as a new standard for inpatient acute mania care.
For now, the result supports clinicians who already use weight-based lithium loading in monitored inpatient settings and gives them a small but specific randomized data point to anchor that practice.
Citation: DOI: 10.1186/s12888-026-08084-z. Moghimi-Sarani et al. Comparative efficacy of lithium carbonate loading dose versus standard dosing, each combined with quetiapine, in acute mania of bipolar I disorder: a randomized single-blind controlled trial. BMC Psychiatry. 2026.
Study Design: Randomized single-blind controlled trial at a psychiatric hospital in Shiraz, Iran.
Sample Size: 60 adult inpatients meeting DSM-5 criteria for bipolar I disorder in the acute manic phase, with a baseline Young Mania Rating Scale score of at least 20.
Key Statistic: Mean YMRS reduction over 14 days was −17.70 in the lithium loading-dose arm versus −13.96 in the standard-titration arm (p < 0.001), with the loading arm reaching therapeutic serum lithium by day 5.
Caveat: Single-center, single-blind, modest sample size; longer-term safety and relapse outcomes are not reported in this trial.