TL;DR: Major depressive disorder and vitiligo may share immune-inflammatory gene signatures. In PLOS One in 2026, the analysis frames MAPK14 as a preliminary candidate marker that still needs clinical and laboratory validation.
Key Findings
- Two public disease datasets were combined: The analysis used 128 major-depression blood samples and 64 controls from GEO, plus a small integrated vitiligo dataset with 15 cases and 15 controls.
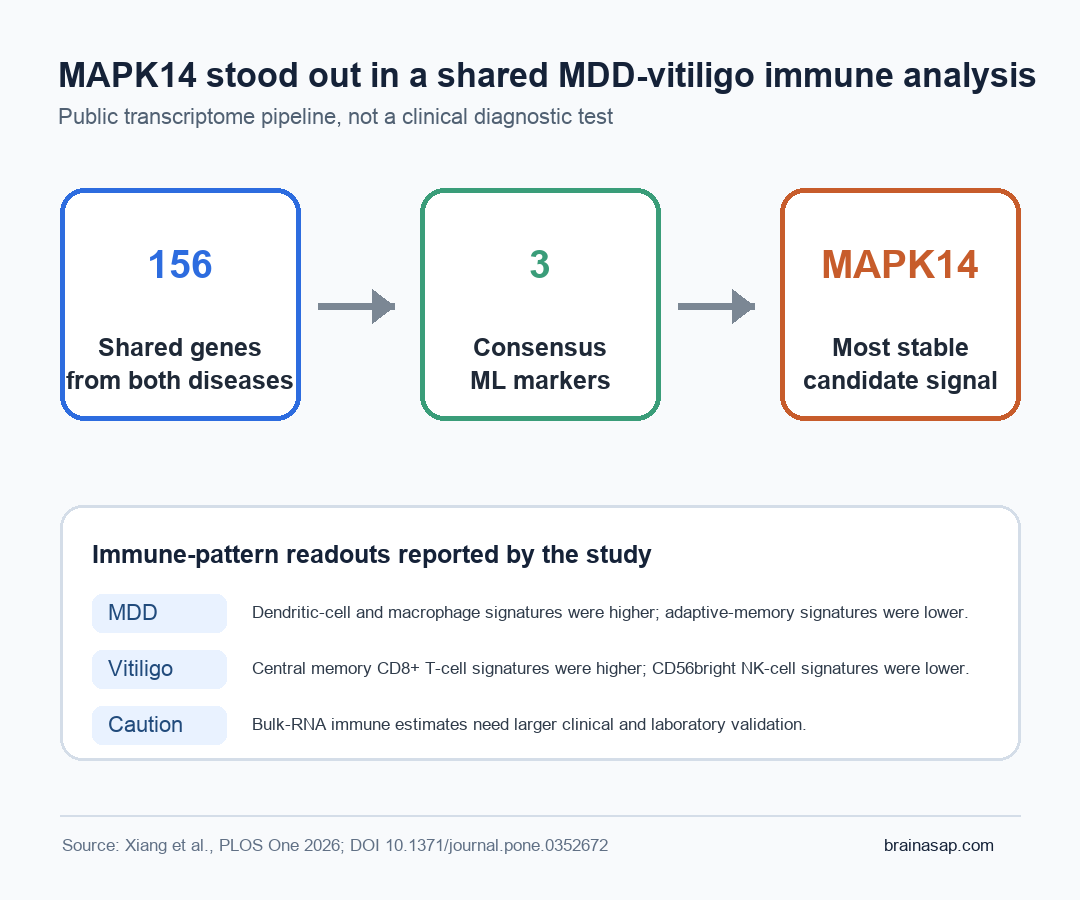
- 156 shared genes were identified: Overlapping differentially expressed genes appeared in major depressive disorder and vitiligo, then narrowed through protein-interaction and enrichment analyses.
- Immune pathways stood out: The 14 hub genes were enriched for immune-response activation, innate immune signaling, leukocyte activation, toll-like receptor signaling, and the IL-17 signaling pathway.
- 3 machine-learning genes survived consensus selection: EXOSC7, KLRG1, and MAPK14 were selected by LASSO, random forest, and SVM-RFE feature-selection methods.
- MAPK14 was the most stable candidate: MAPK14 was upregulated in both disease datasets and kept an AUC above 0.6 across training and validation datasets, but that performance remains exploratory rather than clinically validated.
Source: PLOS One (2026) | Xiang et al.
Vitiligo is usually described as a skin disease, while major depressive disorder is usually described as a psychiatric illness. Researchers tested whether the two conditions also share gene-expression and immune signatures.
The analysis started from the observation that vitiligo and depression often appear together. Some of that overlap is social and psychological: visible depigmentation can carry stigma, stress, and lower quality of life.
But the study argues that the link may not be only reactive distress. Shared immune and inflammatory biology may also help explain why both conditions cluster.
Public Transcriptome Data Linked MDD and Vitiligo
The study used public Gene Expression Omnibus datasets rather than collecting new patient samples. For major depressive disorder, the main dataset included 192 whole-blood samples: 128 from people with MDD and 64 from healthy controls.
The integrated vitiligo discovery data combined 2 smaller datasets, yielding 15 vitiligo samples and 15 controls after batch correction. That small vitiligo sample is a major caveat in the paper, because it limits how confidently the results can generalize.
The first step was broad. The researchers identified 1,707 differentially expressed genes in the MDD dataset and 1,849 in the vitiligo datasets. Intersecting those lists produced 156 co-expressed genes that appeared altered in both conditions.
Those 156 genes became the candidate pool for a protein-protein interaction network. That network highlighted 14 hub genes, including KLRG1, TNF, MAPK14, EXOSC7, IRF4, and EOMES.
Immune and Inflammatory Pathways Stood Out
The enrichment results were the most biologically coherent part of the study. The shared hub genes were tied to immune-response activation, innate immune signaling, leukocyte activation, T-cell differentiation, and toll-like receptor signaling.
The enrichment pattern fits the known biology of both disorders. Vitiligo is an autoimmune disease in which melanocyte loss is shaped by inflammatory and immune-cell activity.
Depression is not an autoimmune disease in the same way. Still, inflammatory signaling, cytokines, glial activation, and peripheral immune changes have all been implicated in at least some MDD subgroups.
The KEGG pathway analysis also highlighted the IL-17 signaling pathway. IL-17 has been discussed in vitiligo biology and in depression-related inflammatory work.
The analysis does not show that IL-17 causes co-occurring vitiligo and depression. It identifies the pathway as a target for follow-up studies.
- Innate immune signaling: The shared gene list pointed toward early inflammatory-response machinery.
- Adaptive immune activity: T-cell-related terms appeared in the enrichment results, fitting vitiligo and immune-mediated skin injury.
- RNA-processing signals: Several enrichment terms involved exosome/RNA degradation machinery, which may reflect broader gene-regulation changes rather than a simple cytokine-only story.
MAPK14 Emerged After 3 Machine-Learning Filters
After narrowing the field to 14 hub genes, the feature-selection stage used LASSO logistic regression, random forest, and SVM-RFE. Only genes selected across all 3 methods were retained as stronger candidates.
That consensus process left EXOSC7, KLRG1, and MAPK14. Among them, MAPK14 received the most attention because it was upregulated in both diseases and showed the most consistent performance across validation datasets.
MAPK14 encodes p38 alpha mitogen-activated protein kinase, part of a stress- and inflammation-responsive signaling pathway. The p38-MAPK pathway can respond to inflammatory cytokines such as TNF-alpha and IL-1, and prior work has connected MAPK14 activity to inflammatory molecule regulation, neuroinflammation, and melanocyte apoptosis.
MAPK14 is biologically plausible. The finding is also easy to overstate.
MAPK14 is not a validated diagnostic blood test or a treatment target ready for clinical use. It is a computationally prioritized gene that requires direct testing.
Immune-Cell Estimates Pointed in Different Directions
The study also used ssGSEA to estimate immune-cell enrichment signatures from bulk RNA data. These are inferred signatures, not direct cell counts, so they should be read as pattern evidence.
In the MDD dataset, enrichment scores for activated dendritic cells and macrophages were higher. Scores for effector memory CD8+ T cells, memory B cells, and type 1 helper T cells were lower.
In the vitiligo dataset, the strongest pattern was different. Central memory CD8+ T-cell signatures were higher, while CD56bright natural killer cell signatures were lower.
That direction fits a skin-autoimmunity signal. The small sample means it still needs confirmation.
The gene-cell correlations added another layer:
- MAPK14 in MDD: It correlated positively with neutrophil signatures and negatively with effector memory CD8+ T-cell signatures.
- MAPK14 in vitiligo: It showed its strongest negative correlation with CD56bright natural killer cell signatures.
- KLRG1 and EXOSC7: These genes also showed immune-cell correlations, supporting the broader immune-microenvironment frame.
The Main Limitation Is Validation, Not Statistics
Researchers applied several statistical and machine-learning checks, including external GEO validation datasets, so the candidate-gene result did not depend on a single discovery dataset alone.
Still, the main limitation is that the study remains computational. It did not measure MAPK14 protein levels in a new clinical cohort or test immune cells from people with both depression and vitiligo.
The study also did not manipulate MAPK14 in a disease model. The analysis used a permissive differential-expression threshold, which can increase false-positive risk.
The vitiligo discovery sample was especially small. Small transcriptomic datasets can produce candidate genes that look convincing until larger cohorts test them under more realistic clinical variation.
The narrow interpretation is that MDD and vitiligo may share immune-inflammatory transcriptomic features, and MAPK14 is a reasonable candidate gene for follow-up. The study helps prioritize experiments, but it does not settle the brain-skin mechanism.
Brain-Skin Research Needs Immune Validation
Research on depression in vitiligo spans dermatology and psychiatry and often emphasizes appearance, stigma, and quality of life.
Those factors are real. Immune biology may also shape vulnerability, persistence, or severity in some patients.
If future studies confirm the MAPK14 and IL-17-related signals in patients who have both conditions, researchers could ask sharper questions.
They could test which inflammatory states predict comorbid depression, whether treatment of skin inflammation changes mood biology, and whether specific immune profiles mark a subgroup that needs integrated dermatology and mental-health care.
For now, the message is cautious but worthwhile. Depression in vitiligo should not be reduced to a psychological reaction alone, and immune biology should not be turned into a diagnostic shortcut.
The useful middle ground is to test whether the brain-skin axis has measurable inflammatory signatures that can improve care without overselling a biomarker before it is ready.
Citation: DOI: 10.1371/journal.pone.0352672. Xiang et al. Bioinformatics analysis reveals the characteristics of immune microenvironment in major depressive disorder and vitiligo. PLOS One. 2026;21(7):e0352672.
Study Design: Integrated bioinformatics analysis of public GEO transcriptomic datasets for major depressive disorder and vitiligo.
Sample Size: Main MDD dataset: 128 MDD samples and 64 controls; integrated vitiligo discovery data: 15 vitiligo samples and 15 controls.
Key Statistic: The study identified 156 shared differentially expressed genes, 14 hub genes, and 3 consensus machine-learning candidates: EXOSC7, KLRG1, and MAPK14.
Caveat: The findings are computational and hypothesis-generating; MAPK14 requires larger clinical cohorts and experimental validation before any clinical use.