TL;DR: A 2026 systematic review and meta-analysis in Musculoskeletal Science and Practice found that people with carpal tunnel syndrome had higher blood markers tied to fibrosis and inflammation, along with lower vitamins and minerals, but the evidence was too heterogeneous for a diagnostic blood test.
Key Findings
- 28-study review: Researchers analyzed 28 studies covering 2,840 carpal tunnel syndrome patients and 6,437 healthy controls.
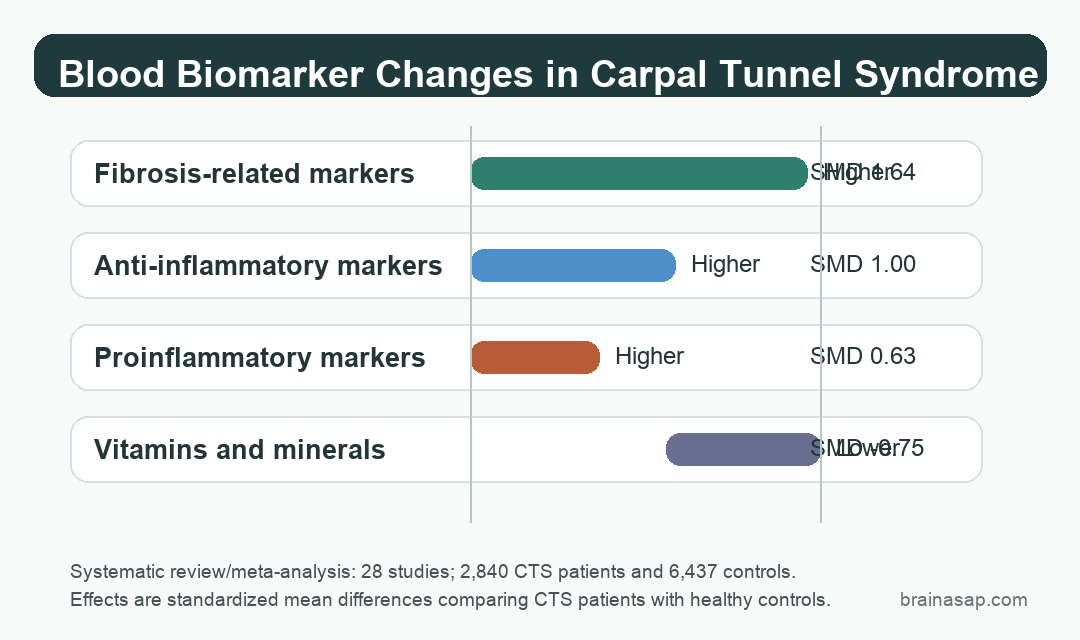
- Fibrosis markers were higher: The largest pooled difference was for fibrosis-related blood markers, with a standardized mean difference of 1.64.
- Inflammatory markers also differed: Proinflammatory markers were higher in CTS, with a pooled standardized mean difference of 0.63.
- Vitamin/mineral levels were lower: The pooled vitamins-and-minerals category was lower in CTS, with a standardized mean difference of -0.75.
- Evidence stayed low-certainty: High heterogeneity and observational designs mean the findings support future mechanism research, not clinical screening.
Source: Musculoskeletal Science and Practice (2026) | Menendez-Camara et al.
Carpal Tunnel Syndrome Showed a Systemic Biomarker Pattern
Carpal tunnel syndrome is usually described as a local compression problem: pressure on the median nerve at the wrist causes numbness, tingling, pain, sensory loss, and sometimes weakness in the hand.
The review tested whether blood markers of inflammation, fibrosis, metabolism, or oxidative stress differed between people with idiopathic CTS and healthy controls. Because the included studies were observational, any differences could reflect contributing biology, consequences of CTS, or other group differences.
Researchers searched seven databases through February 2026 and included observational studies, case-control studies, cohort studies, and baseline measures from trials when they compared quantitative blood biomarkers in idiopathic CTS against healthy controls.
The final evidence set included 28 studies, with 2,840 CTS patients and 6,437 controls. The CTS group averaged about 52 years old and was predominantly female, which matches the known epidemiology of the condition.
- Population: adults with idiopathic carpal tunnel syndrome, not CTS caused by diabetes, dialysis, rheumatoid arthritis, pregnancy, or trauma.
- Comparator: healthy adults without peripheral neuropathy or central nervous system disorders.
- Outcome: quantitative blood biomarkers grouped by inflammation, fibrosis, oxidative stress, vitamins/minerals, immune-cell counts, and related categories.
Fibrosis-Related Markers Had the Largest Pooled Difference
The strongest pooled result involved fibrosis-related markers. Compared with controls, CTS patients had higher levels in this category, with a standardized mean difference of 1.64 and a 95% confidence interval from 0.96 to 2.33.
Fibrosis is relevant because the median nerve does not sit alone in the carpal tunnel. The surrounding subsynovial connective tissue and transverse carpal ligament can become thicker or stiffer, and that tissue environment may affect pressure around the nerve.
The review does not prove that fibrosis biomarkers caused CTS. Many included studies measured biomarkers after CTS was already present, so the direction could run both ways.
Still, the findings support a practical research point: CTS biology may involve more than nerve conduction at the wrist. Blood markers could help future prospective studies sort patients by inflammatory or fibrotic pathway activity.
Inflammation and Vitamin D Moved in Opposite Directions
Inflammatory measures were also higher in CTS. The pooled proinflammatory-marker category showed a standardized mean difference of 0.63, while anti-inflammatory markers also appeared higher, with a standardized mean difference of 1.00.
The mixed immune pattern is not unusual. Blood inflammation is not a single dial.
Some markers rise during inflammatory activation, while counter-regulatory markers may also increase as the body tries to control the response.
At the individual-marker level, higher concentrations were reported for several immune and tissue-response measures:
- Inflammatory chemokines: CCL4, CXCL10, CCL2, and CXCL8 were higher in available comparisons.
- Common inflammation markers: C-reactive protein (CRP), IL-4, and neutrophils were among the altered measures.
- Tissue and oxidative markers: VEGF and malondialdehyde (MDA) were higher, pointing toward vascular and oxidative-stress pathways.
The vitamin/mineral category moved lower, with a pooled standardized mean difference of -0.75. Vitamin D was the clearest individual marker in that direction.
This is not evidence that vitamin D supplementation treats CTS. The review found an association across available studies, not a treatment effect.
Vitamin D status may reflect broader health, inflammation, pain sensitivity, sun exposure, diet, or comorbid risk.
Low Certainty Keeps the Result Out of the Clinic
The most important limitation is the certainty rating. The authors judged the evidence as low certainty, mainly because the included studies were observational, heterogeneous, and often small or methodologically uneven.
The distinction is clinically important. A blood biomarker can be statistically different between groups and still be unusable for diagnosis, prognosis, or treatment selection.
- No causal direction: most studies cannot show whether biomarker changes preceded CTS or followed nerve compression and pain.
- Different assays: biomarker methods, patient selection, and control groups varied across studies.
- Clinical outcomes were thin: the review could summarize associations with symptoms and severity only where studies reported comparable data.
For now, the findings mainly guide future research. Prospective studies could test whether fibrosis, inflammation, oxidative stress, and vitamin D status predict CTS development, symptom severity, recovery after decompression, or treatment response.
CTS Shows a Nerve-Compression Disorder With Whole-Body Clues
Carpal tunnel syndrome still begins with the median nerve at the wrist. The review does not replace clinical examination, nerve conduction testing, ultrasound, or established management.
It does suggest that CTS may not be fully explained by wrist anatomy alone. Across human studies, blood markers related to fibrosis, inflammation, oxidative stress, and vitamin D status differed from controls.
The strongest future version of this work would follow people over time, measure biomarkers before treatment, and connect those measurements to symptoms, nerve conduction, imaging, and recovery. Until then, the finding is mechanistic support, not a clinical blood-test claim.
Citation: DOI: 10.1016/j.msksp.2026.103561. Menendez-Camara et al. Altered blood-based biomarkers in carpal tunnel syndrome. A systematic review and meta-analysis. Musculoskeletal Science and Practice. 2026;84:103561.
Study Design: Systematic review and meta-analysis of observational blood-biomarker studies in idiopathic carpal tunnel syndrome.
Sample Size: 28 studies covering 2,840 CTS patients and 6,437 healthy controls.
Key Statistic: Fibrosis-related markers were higher in CTS, with SMD 1.64 and 95% CI 0.96 to 2.33.
Caveat: The evidence was low-certainty, heterogeneous, and observational, so it cannot establish causality or support a diagnostic blood test.