TL;DR: A 2026 randomized trial in Journal of Medical Internet Research tested the web-based Health Check-Up for Expectant Moms program in 176 pregnant women at risk for substance use or sexually transmitted infection risk, but reductions in alcohol, cannabis, and condomless sex did not differ clearly from an attention-matched control condition.
Key Findings
- 176 pregnant women were randomized: Researchers assigned 88 participants to the Health Check-Up for Expectant Moms (HCEM) and 88 to a time-, attention-, and information-matched control condition.
- Cannabis was the most common substance signal: At baseline, 35.2% of participants reported cannabis use in the prior 90 days, while 10.2% reported use in the month before baseline.
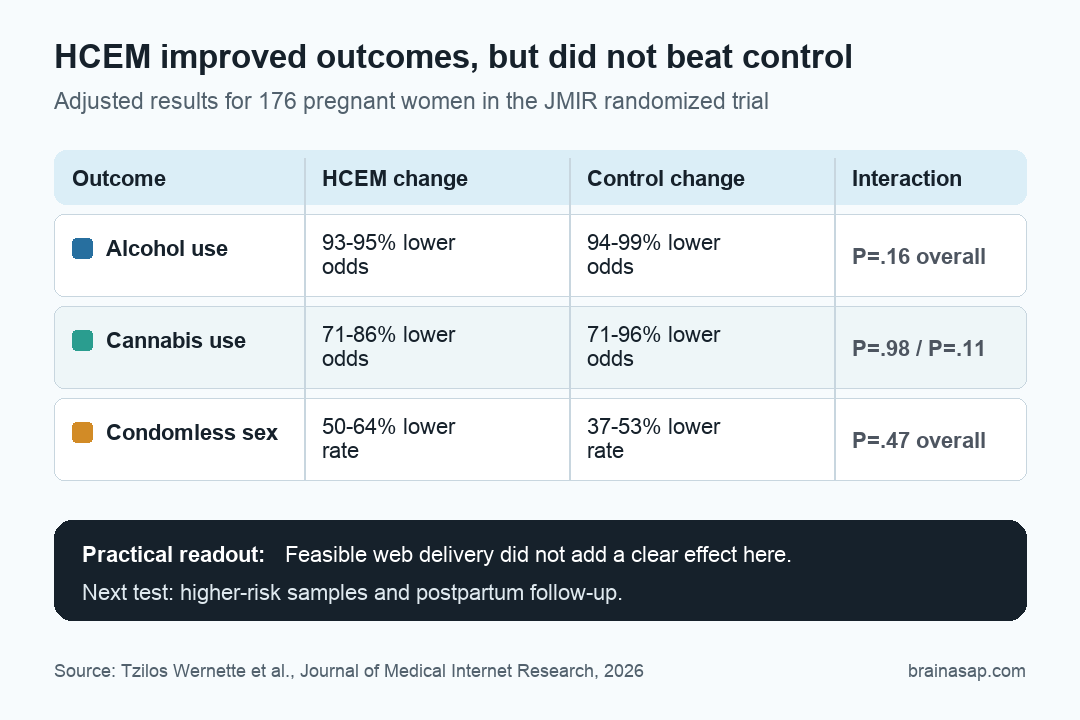
- Alcohol use fell in both groups: Adjusted odds of alcohol use were lower at 2 and 6 months in both HCEM and control arms, but the overall time-by-group interaction was not significant (P=.16).
- Cannabis reductions also did not separate by arm: HCEM and control participants both reported lower cannabis use over time, with no significant arm-by-time difference at 2 months (P=.98) or 6 months (P=.11).
- Condomless sex declined without a clear HCEM-specific pattern: Both groups reported fewer condomless-sex occasions over time, but the overall time-by-group interaction was not significant (P=.47).
Source: Journal of Medical Internet Research (2026) | Tzilos Wernette et al.
Digital pregnancy interventions are appealing for a practical reason: they can let patients answer sensitive questions about alcohol, cannabis, drug use, and sexual risk privately, without waiting for a specialized clinic visit.
This randomized trial tested whether that convenience translated into stronger behavior change. The answer was cautious.
The web-based program was feasible and well matched to prenatal care needs, but it did not clearly outperform an attention-matched control condition on the main self-reported outcomes.
HCEM Tested Motivational Interviewing in a Private Web Format
Health Check-Up for Expectant Moms (HCEM) was built as a fully automated, web-delivered brief intervention. It used a motivational-interviewing style, with a narrator guiding participants through pregnancy-specific information, risk perception, personal motivation, and behavioral skills.
The program had three interactions: an initial session of about 40 minutes, followed by two shorter booster sessions of 15 to 20 minutes. The control condition used the same technology platform and matched HCEM for time, attention, and information, but it did not include the same motivational-interviewing content.
- Substance-use target: Alcohol, drug use, and especially cannabis use during pregnancy.
- Sexual-health target: Condomless sex and sexually transmitted infection risk during the antenatal period.
- Delivery target: A private web format that could work even when in-person prenatal care access is limited.
Recruitment began in Michigan clinics before the SARS-CoV-2 pandemic, then shifted to remote recruitment through phone, text, email, and social media.
That shift matters because the trial was not only testing intervention content. It was also testing a delivery model under real-world constraints.
Pregnancy Itself Was Already Linked to Large Self-Change
The main interpretive problem is visible before the intervention effect is even tested. Baseline alcohol use included both pre-pregnancy and pregnancy use, and many participants had already reduced use by the time they enrolled.
Past-month alcohol use at baseline was only 2.84% overall, even though 65.9% reported at least one drink in the broader 90-day baseline window. That pattern suggests a large amount of spontaneous change after pregnancy recognition.
Cannabis followed a similar but less extreme pattern. At baseline, 35.2% reported cannabis use in the prior 90 days, while 10.2% reported use in the prior month.
By the 6-month follow-up, 8% of participants with data reported cannabis use.
Those changes are clinically important, but they make a trial harder to read. When a low-risk or already-changing sample enters a behavior-change program, the intervention has less room to produce a visible advantage over a well-designed control condition.
Alcohol and Cannabis Use Fell in Both Trial Arms
In adjusted models, alcohol use declined sharply from baseline in both groups. HCEM participants had lower odds of alcohol use at 2 months (AOR 0.07, 95% CI 0.03-0.17) and 6 months (AOR 0.05, 95% CI 0.02-0.12).
The control group also declined at 2 months (AOR 0.06, 95% CI 0.02-0.18) and 6 months (AOR 0.01, 95% CI 0-0.09). The overall time-by-group interaction was P=.16, so the pattern did not show a statistically clear HCEM advantage.
Cannabis showed the same basic structure. HCEM participants had lower adjusted odds at 2 months (AOR 0.29, 95% CI 0.13-0.64) and 6 months (AOR 0.14, 95% CI 0.06-0.37). Control participants also improved at 2 months (AOR 0.29, 95% CI 0.14-0.61) and 6 months (AOR 0.04, 95% CI 0.01-0.13).
Condomless Sex Declined, but the Group Difference Was Unclear
Condomless vaginal sex was common at baseline: 99.4% of participants reported it. That proportion fell to 87.8% at 2 months and 84.1% at 6 months among participants with follow-up data.
The adjusted model showed lower rates over time in both groups. HCEM participants decreased by 50% at 2 months and 64% at 6 months. Control participants decreased by 37% at 2 months and 53% at 6 months.
Even there, the time-by-group interaction did not support a clear differential pattern. The overall interaction was P=.47, with nonsignificant interaction terms at both follow-up points.
- Alcohol outcome: Strong within-arm reductions, no significant overall HCEM-specific change pattern.
- Cannabis outcome: Strong within-arm reductions, no significant 2-month or 6-month arm-by-time difference.
- Condomless-sex outcome: Declines in both groups, no significant overall interaction.
Low Baseline Risk and Missing Follow-Up Limited the Test
The trial does not show that digital prenatal behavioral support is useless. It shows that this version of HCEM did not beat a strong control condition in this sample.
Several limits make that distinction important. The sample was relatively small, highly educated, geographically limited to one Midwestern state, and lower risk than the intervention question ideally needed.
A total of 35% of participants missed the 6-month follow-up, largely because they gave birth before the target assessment date.
Biological samples for drug use were also incomplete because of pandemic restrictions. Missing objective data rose from 30% at baseline to 55% at the 6-month follow-up, leaving the main efficacy readout heavily dependent on self-report.
A private web intervention may still help deliver education, reduce stigma, and extend support in maternity-care deserts, but this trial did not show that HCEM improved the measured behaviors more than the matched control.
Future trials need higher-risk samples, stronger postpartum follow-up, and enough room for measurable change beyond pregnancy-related self-change.
Citation: DOI: 10.2196/95944. Tzilos Wernette et al. A Web-Based Intervention for Reducing Sexually Transmitted Infections and Substance Use During Pregnancy: Randomized Controlled Trial. Journal of Medical Internet Research. 2026;28:e95944.
Study Design: Randomized controlled trial of a web-based motivational-interviewing intervention versus an attention-, time-, and information-matched control condition.
Sample Size: 176 pregnant women in Michigan randomized 1:1 to HCEM or control, with follow-up at 2 and 6 months after baseline.
Key Statistic: Alcohol, cannabis, and condomless-sex outcomes improved over time, but time-by-group interaction tests were not significant: alcohol P=.16, cannabis 2-month P=.98 and 6-month P=.11, condomless sex P=.47.
Caveat: Low current substance-use frequency, pandemic-era recruitment changes, missing biological samples, and 35% missed 6-month follow-up limited the ability to detect an intervention-specific effect.