TL;DR: A 2026 review in Annals of Medicine argues that circadian rhythm disruption in major depressive disorder (MDD) reaches beyond poor sleep, linking clock-gene variation, sleep-wake timing, stress-hormone rhythms, melatonin signaling, and chronotherapy targets.
Key Findings
- 264 million affected: The review frames MDD as a leading global disability cause affecting more than 264 million people.
- 50-90% sleep disruption: Sleep-wake disruption is described as common in MDD, affecting roughly half to nearly all patients depending on the cohort and definition.
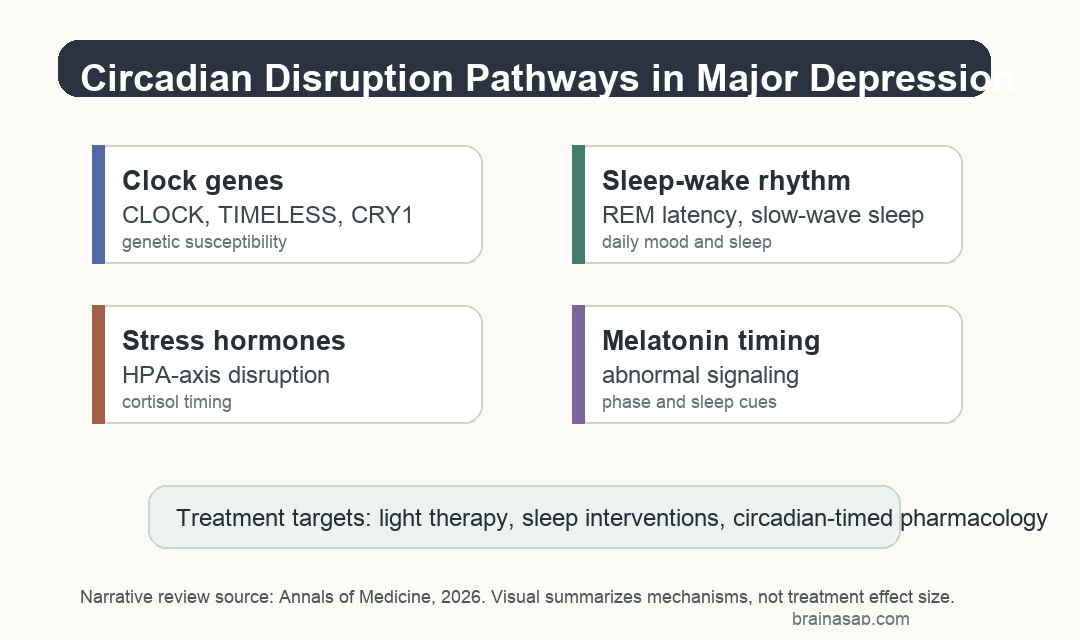
- Clock genes were highlighted: CLOCK, TIMELESS, and CRY1 were named as core circadian genes linked to disruption and MDD susceptibility.
- Stress timing mattered: Dysregulated hypothalamus-pituitary-adrenal (HPA) axis function was presented as one route connecting circadian timing with depression biology.
- Chronotherapy stayed targeted: Light therapy, sleep interventions, and timing-based pharmacology were reviewed as treatment directions, not universal substitutes for standard care.
Source: Annals of Medicine (2026) | Saeed et al.
Circadian Rhythm Disruption Was Framed as Depression Biology
Major depressive disorder (MDD) can involve changes in sleep timing, daily hormone rhythms, melatonin signaling, and clock-gene pathways, in addition to mood and cognitive symptoms.
Circadian rhythms are the body’s roughly daily cycles in sleep, hormone release, metabolism, body temperature, alertness, and mood. In depression, those cycles can shift, flatten, fragment, or lose coordination with light-dark timing.
The review does not treat circadian disruption as only a symptom that follows low mood. The authors summarize genetic, clinical, experimental, and therapeutic evidence suggesting that timing-system disruption may help drive MDD in some patients.
That distinction changes the clinical question. If circadian disruption contributes to depression biology, then sleep timing, light exposure, melatonin timing, and clock-gene pathways become treatment-relevant variables rather than background lifestyle details.
Sleep-Wake Changes Covered More Than Insomnia
The sleep section goes beyond a simple insomnia description. The review describes sleep-wake disruption as very common in MDD, with estimates ranging from 50% to 90% of patients depending on the study and symptom definition.
Depression-related sleep disruption can include trouble falling asleep, early morning awakening, daytime sleepiness, frequent nighttime waking, nightmares, and altered sleep architecture.
Several sleep measures were described as relevant to MDD biology:
- REM sleep latency: rapid eye movement sleep can begin earlier than expected in many depressed patients.
- Slow-wave sleep: deep non-REM sleep activity is often reduced, which may weaken sleep homeostasis.
- Diurnal mood variation: symptoms may be worse in the morning or evening, depending partly on chronotype and circadian phase.
The review also notes that sleep deprivation can produce rapid antidepressant effects in some patients. That does not make sleep loss a practical long-term treatment, but it shows how tightly mood can respond to shifts in sleep pressure and circadian timing.
CLOCK, TIMELESS, and CRY1 Connected Timing Genes to MDD
Clock genes help cells keep time. They regulate molecular feedback loops that synchronize many tissues with the central clock in the suprachiasmatic nucleus, a timing hub in the hypothalamus.
The review highlights CLOCK, TIMELESS, and CRY1 as genes linked to circadian disruption and MDD susceptibility. These associations do not mean a single gene explains depression.
The stronger interpretation is pathway-level. Genetic variation may shift sleep timing, light sensitivity, hormone rhythms, and mood regulation in ways that make some people more vulnerable when stress, inflammation, social timing, or sleep loss are present.
- CLOCK: a core timing regulator tied to circadian rhythm generation.
- TIMELESS: part of the molecular machinery that helps maintain circadian cycling.
- CRY1: a cryptochrome gene involved in feedback control of the biological clock.
Stress Hormones and Melatonin Added Biological Timing Layers
The review also emphasizes the hypothalamus-pituitary-adrenal (HPA) axis, the stress-hormone system that helps regulate cortisol timing. Cortisol normally follows a daily rhythm, with a morning peak and lower evening levels.
In MDD, HPA-axis timing can become dysregulated. A mistimed or overactive stress-hormone rhythm can affect sleep, immune signaling, metabolism, emotional reactivity, and energy regulation.
Melatonin adds another timing layer. It normally rises in the evening, helping the brain and body interpret darkness and prepare for sleep.
Abnormal melatonin signaling can shift circadian phase or weaken the sleep-wake cue.
These pathways are not separate boxes in real patients. Sleep timing, stress hormones, melatonin, light exposure, social schedules, and medication timing can interact.
Chronotherapy Requires Matching the Patient’s Timing Problem
Chronotherapeutic approaches try to correct, shift, or stabilize biological timing. The most familiar examples are bright light therapy, sleep interventions, and carefully timed medication strategies.
The review does not support a one-size-fits-all timing prescription for depression. A patient with delayed sleep phase, morning-worst mood, evening-worst mood, shift-work disruption, or insomnia-dominant depression may need different timing targets.
- Light therapy: may help when light exposure and circadian phase are part of the depressive pattern.
- Sleep interventions: can target insomnia, sleep regularity, and daily rhythm stabilization.
- Timed pharmacology: may become more useful if genetic or molecular markers identify circadian subtypes.
Timing also affects measurement. A cortisol sample, sleep diary, actigraphy record, or melatonin assessment can mean different things depending on clock time, work schedule, light exposure, and recent sleep.
That is why timing-aware depression care needs more than asking whether a patient sleeps poorly. It needs the pattern: when sleep starts, when mood is worst, when light exposure happens, and whether the daily rhythm is stable or drifting.
The practical clinical message is measured: circadian biology may help personalize MDD treatment, but the review is not a completed comparative trial. It points toward better patient stratification and timing-aware care.
Citation: DOI: 10.1080/07853890.2026.2671594. Saeed et al. Circadian rhythms in major depressive disorder: mechanistic insights and therapeutic frontiers. Annals of Medicine. 2026;58:2671594.
Study Design: Narrative review of genetic, clinical, mechanistic, and therapeutic evidence on circadian rhythm disruption in MDD.
Sample Size: Not a pooled patient sample; this is a narrative synthesis of prior genetic, clinical, mechanistic, and therapeutic evidence.
Key Statistic: The review reports sleep-wake disruption in roughly 50-90% of MDD patients and cites more than 264 million people affected by MDD worldwide.
Caveat: As a review, it summarizes mechanisms and treatment directions rather than estimating one causal effect or testing one chronotherapy protocol.