TL;DR: A 2026 randomized phase 2b trial in Journal of Clinical Psychopharmacology found that the PDE10A inhibitor MK-8189 did not improve Positive and Negative Syndrome Scale (PANSS) schizophrenia symptom scores more than placebo after 6 weeks, while risperidone separated from placebo in the same trial.
Key Findings
- 458 treated participants: The acute phase included 132 people on MK-8189 16 mg, 132 on MK-8189 24 mg, 65 on risperidone 6 mg, and 129 on placebo.
- Primary symptom scale: The main endpoint was change in PANSS total score, a standard schizophrenia symptom scale, from baseline to week 6.
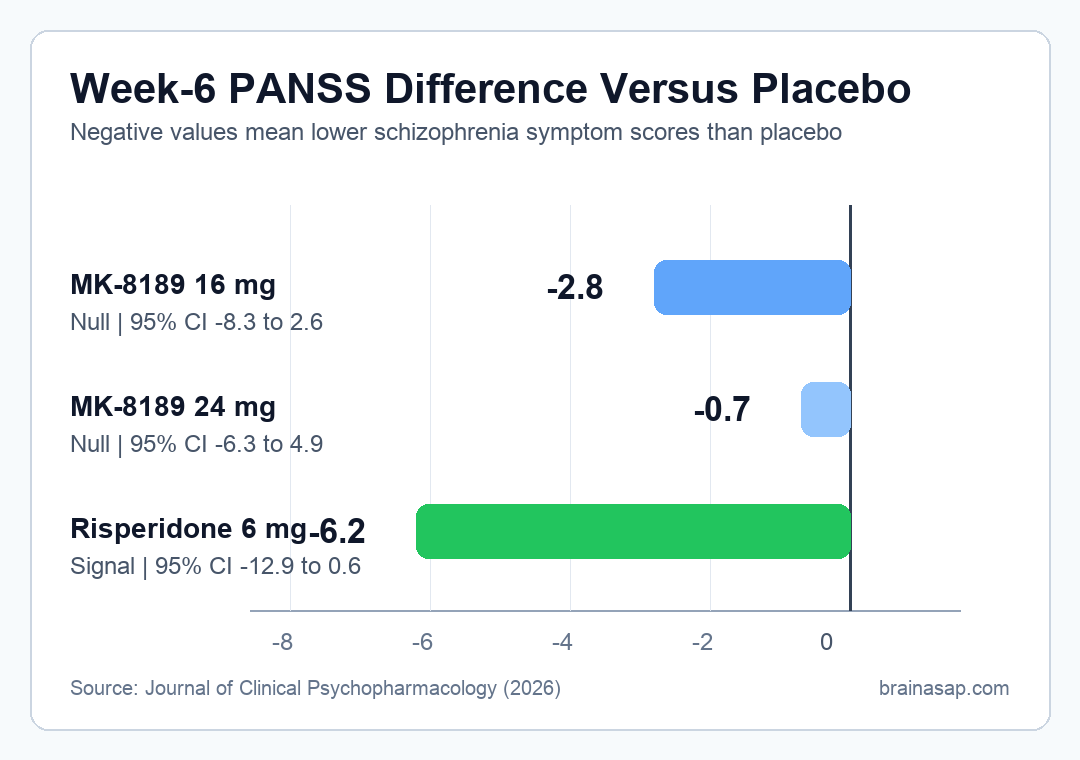
- 16 mg null result: MK-8189 16 mg differed from placebo by -2.8 PANSS points (95% CI, -8.3 to 2.6; P = 0.241).
- 24 mg null result: MK-8189 24 mg differed from placebo by -0.7 PANSS points (95% CI, -6.3 to 4.9; P = 0.784).
- Assay sensitivity: Risperidone separated from placebo by -6.2 PANSS points (95% CI, -12.9 to 0.6; P = 0.040), showing the trial could detect an antipsychotic signal.
Source: Journal of Clinical Psychopharmacology (2026) | Mukai et al.
MK-8189 was designed to test whether phosphodiesterase 10A (PDE10A) inhibition could treat acute schizophrenia symptoms without working like a direct dopamine D2 blocker. PDE10A is concentrated in striatal medium spiny neurons, a circuit target tied to dopamine signaling and antipsychotic pharmacology.
The trial tested that mechanism more directly than earlier work. Researchers used higher MK-8189 doses, longer treatment, and an active risperidone arm so the negative result would be easier to interpret.
MK-8189 16 mg and 24 mg Did Not Beat Placebo on PANSS
The main question was whether 6 weeks of MK-8189 improved total scores on the Positive and Negative Syndrome Scale (PANSS), which combines positive symptoms, negative symptoms, and general psychopathology in schizophrenia trials.
Neither tested MK-8189 dose showed a statistically significant advantage over placebo. The 16 mg group had a placebo-adjusted difference of -2.8 PANSS points, and the 24 mg group had a difference of -0.7 PANSS points.
- 16 mg MK-8189: The confidence interval ranged from -8.3 to 2.6 points, so the estimate did not clearly exclude no benefit.
- 24 mg MK-8189: The confidence interval ranged from -6.3 to 4.9 points, giving an even smaller central estimate.
- Primary endpoint: The trial was judged on week-6 PANSS total-score change, not only early symptom movement.
The result matters because the 24 mg dose was expected to produce about 80% sustained PDE10A enzyme occupancy. If higher continuous target engagement were enough to produce antipsychotic efficacy, this was the dose most likely to show it.
Risperidone Confirmed the Trial Could Detect a Schizophrenia Drug Effect
The study included risperidone 6 mg as an active comparator for assay sensitivity. That means the trial was not only asking whether MK-8189 worked; it also asked whether the study setup could detect a known antipsychotic effect.
Risperidone separated from placebo by -6.2 PANSS points at week 6. That active-control result supports the interpretation that MK-8189 itself failed to show the expected symptom benefit.
- Placebo comparison: MK-8189 was tested against placebo at two higher doses.
- Active-control check: Risperidone provided a benchmark for whether symptom ratings could move in the expected direction.
- Mechanism test: The design asked whether PDE10A inhibition alone could act like a clinically useful antipsychotic strategy.
PANSS findings were negative for acute psychosis. The trial does not prove every possible PDE10A strategy is useless, but it weakens the case for MK-8189 as a standalone antipsychotic at these doses.
Higher PDE10A Target Engagement Still Produced a Null Result
The biological rationale for MK-8189 was plausible. PDE10A regulates cAMP and cGMP signaling in striatal neurons, and modifying those pathways could theoretically influence circuits involved in psychosis.
Earlier PDE10A trials had produced mixed signals, including a prior MK-8189 phase 2a study with initial evidence at 12 mg over 4 weeks. This phase 2b study tested whether 16 mg and 24 mg over a longer period would produce a clearer treatment effect.
- Longer exposure: The acute treatment phase lasted 6 weeks, compared with the 4-week MK-8189 proof-of-concept study described by the researchers.
- Higher doses: The key MK-8189 arms used 16 mg and 24 mg, with an 8 mg arm dropped after partial enrollment.
- Stronger target engagement: The 24 mg dose was predicted to produce roughly 80% sustained enzyme occupancy.
Those design choices make the null result clinically important. The trial tested a more intensive version of the mechanism and still did not show a PANSS advantage.
Adverse-Event Dropouts Were Highest With MK-8189 24 mg
Tolerability also mattered because the higher dose was the best chance to test the target-engagement hypothesis. During the acute phase, discontinuation due to an adverse event occurred in 25.0% of participants assigned to MK-8189 24 mg.
The corresponding rates were lower in the other groups: 12.9% with MK-8189 16 mg, 12.3% with risperidone, and 12.4% with placebo.
- High-dose tradeoff: The dose most likely to maximize PDE10A occupancy had the highest adverse-event discontinuation rate.
- Weight and metabolic measures: The report noted MK-8189-related weight reduction and some decreases in lipids, while other vital-sign changes were broadly comparable.
- Clinical boundary: Better metabolic signals would not offset a failed antipsychotic endpoint in acute schizophrenia.
For drug development, the dose-response profile is unfavorable. A higher dose did not produce stronger efficacy, and it came with more treatment discontinuation.
The Trial Leaves Cognitive and Negative Symptoms Less Settled
The supported conclusion is specific: PDE10A inhibition with MK-8189 did not improve acute psychotic symptoms on PANSS total score at the tested doses. PANSS is important, but it is not a complete map of schizophrenia.
The researchers noted that the design was not built to robustly test cognition or negative symptoms with specialized endpoints. Smaller PANSS effects also cannot be fully excluded because the study was powered for a moderate effect.
- Best-supported conclusion: MK-8189 did not show antipsychotic efficacy for an acute schizophrenia episode in this phase 2b design.
- Unresolved domain: Cognitive impairment and negative symptoms would need different trial designs and outcome measures.
- Development implication: A mechanism with strong preclinical logic still needs clear clinical separation from placebo.
For patients and clinicians, the result should not be generalized to every non-D2 schizophrenia approach. It shows that this specific PDE10A inhibitor, at these higher doses and 6-week timing, did not produce the symptom benefit needed for an acute antipsychotic claim.
Citation: DOI: 10.1097/JCP.0000000000002152. Mukai et al. Phase 2b Trial of the PDE10A Inhibitor MK-8189 in People With an Acute Episode of Schizophrenia. Journal of Clinical Psychopharmacology. 2026;46:311-319.
Study Design: Randomized, double-blind phase 2b trial with placebo and risperidone active-control arms.
Sample Size: 458 treated participants in the acute 6-week period across MK-8189, risperidone, and placebo groups.
Key Statistic: MK-8189 16 mg and 24 mg differed from placebo by -2.8 and -0.7 PANSS points, while risperidone differed by -6.2 points.
Caveat: The trial focused on acute PANSS total-score change and did not robustly test cognition or negative symptoms with specialized designs.





