
TL;DR: A 2026 cross-sectional study in BMC Geriatrics found that 43.9% of 945 older adults in Nepal’s Sudurpaschim Province screened positive for geriatric depression, and depression was linked to lower quality-of-life scores across every WHOQoL-8 domain.
Key Findings
- Large household sample: Researchers interviewed 945 adults aged 60 years and older in Hill and Tarai districts of Sudurpaschim Province, Nepal.
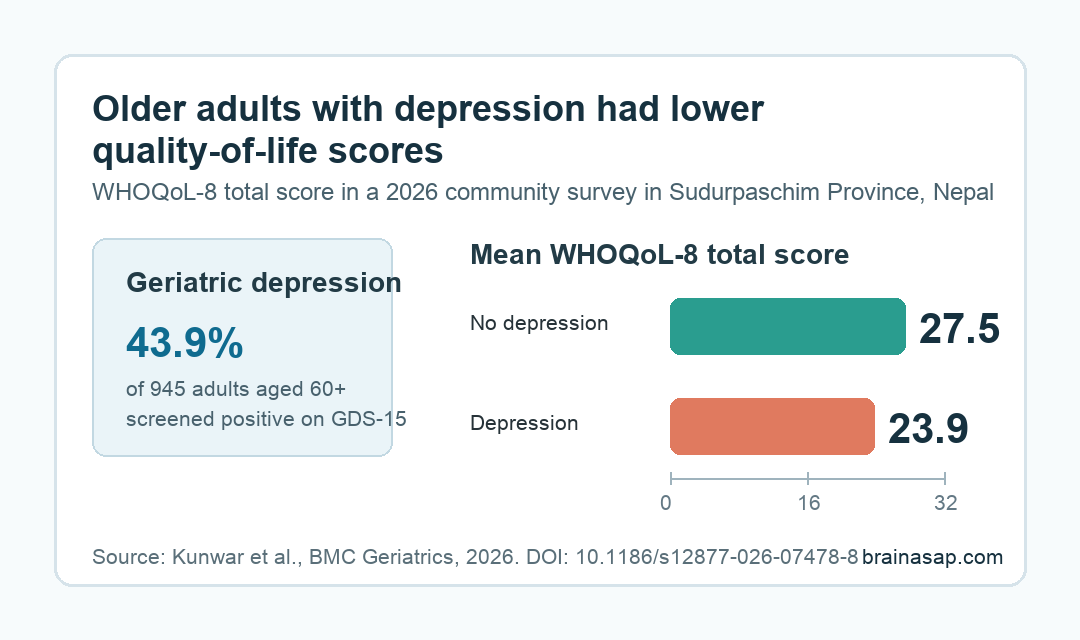
- Depression was common: The Geriatric Depression Scale-15 (GDS-15), a short depression-symptom screen for older adults, identified geriatric depression in 43.9% of participants.
- Two factors remained linked after adjustment: Age 75 years and older had an adjusted odds ratio of 1.5, and Hill-region residence had an adjusted odds ratio of 1.6.
- Quality of life was lower with depression: Participants with depression had a mean total WHOQoL-8 score of 23.9, compared with 27.5 among those without depression.
- Causal claims are limited: The study was cross-sectional and did not include Himalayan districts, so it cannot prove depression caused lower quality of life across the whole province.
Source: Kunwar et al. 2026 BMC Geriatrics study.
Older-adult depression is often discussed as a clinical diagnosis, but this study treated it as a public-health signal. Researchers went door to door in a far-western Nepali province and asked whether depression symptoms were tied to daily quality of life.
The prevalence was high. In a community sample of 945 older adults, nearly 44 in 100 screened positive for geriatric depression.
Those participants also reported lower well-being across physical, psychological, social, and environmental parts of life.
The result should not be read as proof that every older adult with a low quality-of-life score had depression, or that depression caused every quality-of-life difference. It does show that mental health was closely connected with ordinary functioning in this sample.
Sudurpaschim Survey Found 43.9% Geriatric Depression
The study was a cross-sectional household survey conducted from October to December 2021 in Sudurpaschim Province, Nepal. Researchers used multistage random cluster sampling and selected one Hill district and one Tarai district.
Participants were 60 years and older, permanent residents of selected wards, and able to communicate in Nepali. The final participation rate was 98.8%, with 945 of 956 selected older adults taking part.
The sample had several features that matter for interpreting the result:
- Age: The mean age was 69.3 years, and 22.1% were 75 years or older.
- Region: 52.5% lived in the Tarai region, while 47.5% lived in the Hill region.
- Education and work: 65.5% had no formal education, and 97.9% were not formally employed.
- Income: 87.1% reported monthly income at or below 20,000 Nepalese rupees.
Depression was measured with the Geriatric Depression Scale-15 (GDS-15), a 15-item yes/no symptom screen designed for older adults. The Nepali version used a 5/6 cutoff, meaning scores above that threshold counted as likely depression in this study.
Quality of life was measured with the World Health Organization Quality of Life-8 (WHOQoL-8), an eight-item measure covering subjective well-being, physical well-being, psychosocial well-being, and environmental circumstances.
Age 75 and Hill Residence Stayed Linked After Adjustment
The clearest demographic pattern was age. Depression prevalence was 53.6% among participants aged 75 years and older, compared with 41.2% among those younger than 75.
Region also mattered. Depression prevalence was 56.3% among Hill-region residents and 32.7% among Tarai-region residents.
Several variables were associated with depression in the simpler bivariate analyses, including sex, lower income, non-smoking, no alcohol use, and comorbid medical conditions. After multivariable adjustment, the study’s strongest retained signals were narrower:
- Age 75 years and older: adjusted odds ratio 1.5, with a 95% confidence interval of 1.1 to 2.2.
- Hill-region residence: adjusted odds ratio 1.6, with a 95% confidence interval of 1.1 to 2.1.
This distinction is important. A raw percentage can show where depression was more common, but adjusted odds ratios show which associations remained after the model considered several factors together.
The study does not identify why Hill-region residence was linked to higher depression odds. Geography may stand in for access to care, income, transport, social support, or other unmeasured conditions.
Depression Tracked Lower WHOQoL-8 Scores
The quality-of-life result was the most consistent part of the paper. Participants with depression had a mean total WHOQoL-8 score of 23.9, while those without depression had a mean score of 27.5.
Higher WHOQoL-8 scores indicate better quality of life, so that gap points in the expected direction: depression symptoms were linked to worse reported daily life.
The relationship was not confined to one domain. Total GDS-15 depression scores had a negative correlation of -0.48 with total quality-of-life scores, and all four WHOQoL-8 domains were lower as depression scores rose.
The domain correlations were strongest for physical well-being:
- Physical well-being: correlation -0.49 with depression score.
- Subjective well-being: correlation -0.38.
- Psychosocial well-being: correlation -0.38.
- Environmental circumstances: correlation -0.23.
This does not prove that depression caused the physical quality-of-life difference. Poor health, disability, pain, social isolation, and poverty can all move in both directions with depression.
The clinical implication is that depression screening and quality-of-life assessment should not be separated too sharply in older-adult care.
Cross-Sectional Data Limit the Causal Claim
The study has useful strengths: a large community sample, face-to-face interviews, culturally adapted Nepali instruments, and a very high participation rate.
The limits are just as important. Researchers did not include the Himalayan districts of Sudurpaschim Province, so the sample does not fully represent every ecological region.
The design was also cross-sectional, meaning depression symptoms and quality-of-life scores were measured at the same general time.
Several missing variables could matter. The study did not deeply measure marital status, family support, neighborhood support, physical exercise, biometric health, or access to health care.
Those factors could partly explain why depression and lower quality of life appeared together.
Still, the finding is not a small signal. In this surveyed population, geriatric depression was common, and it was linked with lower scores in every measured quality-of-life domain.
For health systems, the narrow takeaway is practical: older adults in under-resourced regions may need depression screening alongside questions about physical functioning, social support, income strain, and daily living conditions.
Citation: DOI: 10.1186/s12877-026-07478-8. Kunwar et al. Depression and quality of life (QoL) among older adults in Sudurpashchim Province, Nepal: findings from a cross-sectional community survey. BMC Geriatrics. 2026.
Study Design: Cross-sectional community household survey in two selected districts of Sudurpaschim Province, Nepal.
Sample Size: 945 adults aged 60 years and older.
Key Statistic: Geriatric depression prevalence was 43.9%, and mean WHOQoL-8 total score was 23.9 with depression versus 27.5 without depression.
Caveat: Cross-sectional data cannot prove causality, and Himalayan districts were not included.





