TL;DR: A 2026 retrospective ICU study in the International Journal of General Medicine found that 24-hour open visiting was associated with lower delirium incidence and lower anxiety/depression scores than 1-hour restricted visiting in chronic critically ill patients.
Key Findings
- 264 ICU patients: The retrospective cohort included 132 restricted-visiting patients and 132 open-visiting patients.
- 24-hour access: The open-visiting group allowed family access around the clock, while restricted visiting allowed 1 hour daily.
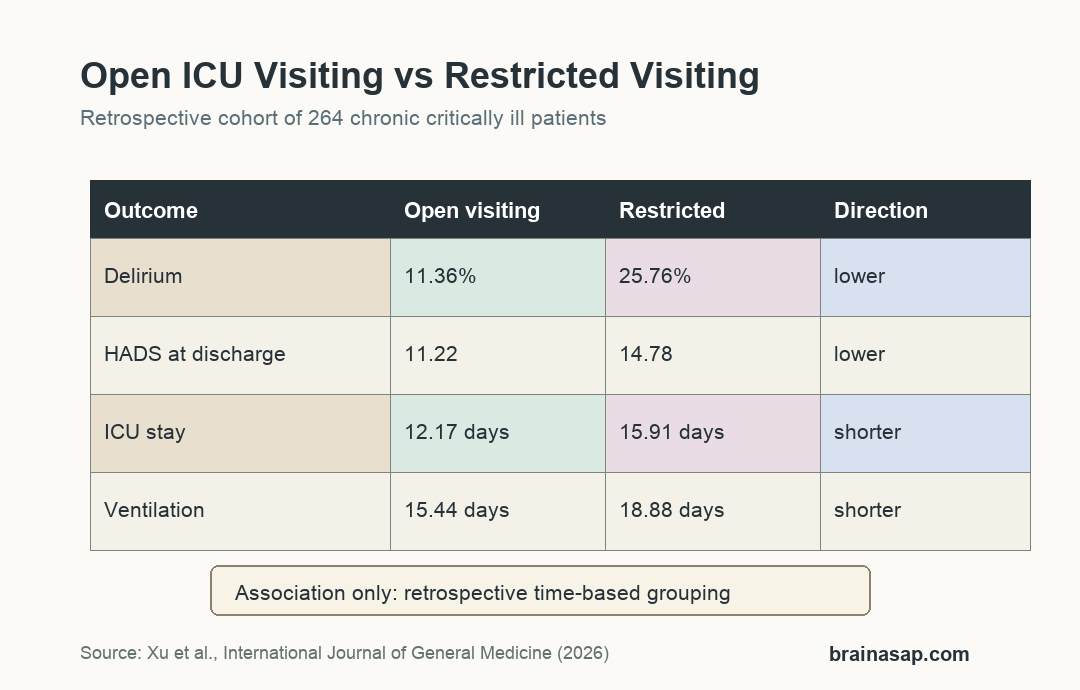
- Delirium fell: Delirium incidence was 11.36% with open visiting versus 25.76% with restricted visiting.
- HADS scores were lower: Discharge Hospital Anxiety and Depression Scale scores were 11.22 versus 14.78 points.
- ICU stay shortened: ICU stay averaged 12.17 days with open visiting versus 15.91 days with restricted visiting.
Source: International Journal of General Medicine (2026) | Xu et al.
Open ICU Visiting Was Tested in Chronic Critical Illness
ICU delirium is an acute disturbance in attention, awareness, and thinking that can develop during critical illness. It is clinically important because delirium can complicate recovery, prolong hospitalization, and sometimes leave patients with lasting cognitive problems.
This study focused on chronic critically ill ICU patients, defined here as patients with ICU stay of at least 7 days and persistent serious illness. That group is vulnerable to loneliness, anxiety, sleep disruption, sedation exposure, and prolonged mechanical ventilation.
Researchers compared 2 visiting policies at a tertiary hospital ICU in China. The restricted-visiting group received a fixed 1-hour daily visit, while the open-visiting group allowed family members to enter at any time under infection-control rules.
- Restricted visiting: 132 patients with 1 hour of daily family access.
- Open visiting: 132 patients with 24-hour family access and bedside guidance.
- Main brain outcome: delirium assessed with the Confusion Assessment Method for the ICU (CAM-ICU).
Eligibility required age of at least 18 years, ICU stay of at least 7 days, and a clear diagnosis of chronic critical illness. Patients with expected survival under 24 hours, severe multidrug-resistant infection, death, or ICU transfer during the study period were excluded.
Delirium Was Lower With 24-Hour Family Access
The delirium result was the clearest brain-related outcome. In the open-visiting group, 15 of 132 patients developed delirium, or 11.36%.
In the restricted-visiting group, 34 of 132 patients developed delirium, or 25.76%. The difference was statistically significant, with P < 0.05.
The study also reported that CAM-ICU assessments were performed twice daily by trained ICU nurses, with positive findings verified by a senior intensivist. Inter-rater reliability training produced a reported kappa coefficient of 0.85.
- Open group: 11.36% delirium incidence.
- Restricted group: 25.76% delirium incidence.
- Assessment method: twice-daily CAM-ICU screening with senior confirmation for positive findings.
Anxiety and Depression Scores Improved by Discharge
The Hospital Anxiety and Depression Scale (HADS), a screening questionnaire for anxiety and depression symptoms, was similar between groups on the first ICU day. Admission scores were 17.85 in the restricted group and 17.94 in the open group.
At discharge, HADS scores were lower in the open-visiting group: 11.22 versus 14.78 points. Family anxiety scores also favored open visiting, with lower state anxiety and trait anxiety scores among family members.
The family-anxiety result matters because ICU distress is not limited to patients. Family members often help with communication, orientation, motivation, and later recovery planning.
- Patient HADS: 11.22 versus 14.78 points at discharge.
- Family state anxiety: 44.23 versus 56.89 points.
- Family trait anxiety: 44.18 versus 57.54 points.
Ventilation and Hospital Time Were Shorter in the Open-Visiting Group
Open visiting was also associated with shorter clinical recovery measures. Mechanical ventilation lasted 15.44 days in the open group versus 18.88 days in the restricted group.
ICU stay averaged 12.17 days with open visiting and 15.91 days with restricted visiting. Total hospital stay was 20.22 days versus 25.11 days.
Treatment compliance was higher with open visiting, at 89.39% versus 75.45%. The study defined compliance as completion of at least 80% of prescribed therapeutic interventions, including medication, early mobilization, and respiratory therapy.
Air quality did not differ significantly between groups, at 13.17 versus 13.21 cfu/cm2. Visitors in the open model used shoe covers, masks, hand hygiene, and nursing-supervised infection-control procedures.
That infection-control detail is important because open visiting is often resisted on safety grounds. This study suggests structured visiting can be tested without assuming family presence automatically worsens the ICU environment.
Single-Center Retrospective Design Limits the ICU Visiting Claim
The result fits a plausible clinical mechanism: family presence may support orientation, reduce distress, improve communication, encourage treatment participation, and help staff notice mental-status changes. It also fits broader ICU delirium prevention work that emphasizes sleep, orientation, pain control, and non-drug support.
The study did not randomly assign patients at the same time. Grouping was based on policy implementation, which creates risk of temporal confounding from staffing, practice, patient mix, or other unmeasured changes.
- Single center: all patients came from 1 hospital ICU.
- Time cutoff: open visiting began after a policy change rather than concurrent randomization.
- No long-term outcomes: 1-year survival, quality of life, readmission, and patient-reported outcomes were not measured.
- Local culture: family participation in Chinese tertiary hospitals may affect feasibility and results.
Under those limits, the finding supports further prospective ICU visiting trials. It does not prove that every ICU can switch to 24-hour visiting without careful staffing, privacy, and infection-control planning.
Citation: DOI: 10.2147/IJGM.S595535. Xu et al. Comparison of Open Visiting and Restricted Visiting in ICU Chronic Critical Patients: Effects on Negative Emotions and Delirium. International Journal of General Medicine. 2026;19:595535.
Study Design: Single-center retrospective cohort comparison before and after an ICU visiting-policy change.
Sample Size: 264 chronic critically ill ICU patients, with 132 patients per visiting-policy group.
Key Statistic: Delirium incidence was 11.36% with open visiting versus 25.76% with restricted visiting.
Caveat: Time-based retrospective grouping means unmeasured changes besides visiting policy may have contributed to the results.





