TL;DR: A 2026 trial in Journal of Psychopharmacology found that repeated supervised psilocybin sessions reduced Yale-Brown Obsessive Compulsive Scale (YBOCS) scores, a standard measure of obsession and compulsion severity, in 15 adults with OCD.
Key Findings
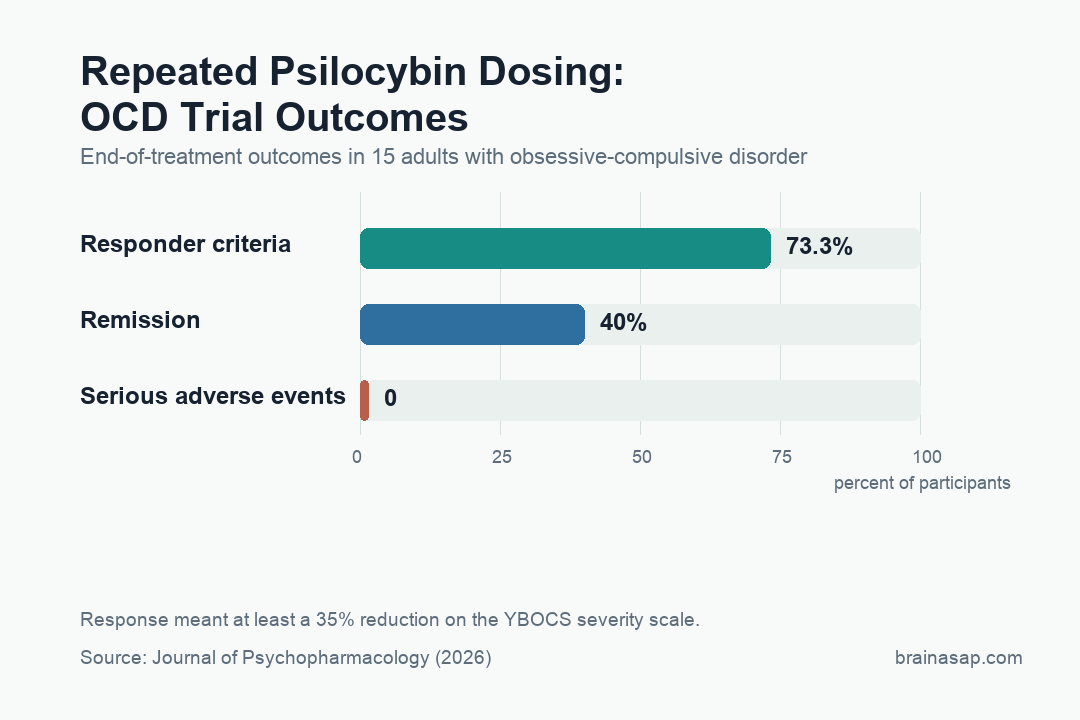
- 73.3% met responder criteria: At the end of the 8-week treatment, 11 of 15 participants had at least a 35% reduction in YBOCS scores.
- 40% reached remission: Six of 15 participants were in remission after receiving at least four high-dose psilocybin sessions.
- Psilocybin reduced YBOCS; lorazepam did not: In the double-blind phase, psilocybin but not active placebo significantly reduced OCD severity.
- No serious safety signal emerged: The paper reports no serious adverse events, no psychotic symptoms, and no significant changes in suicide-severity scores.
- Durability and dose remained exploratory: Follow-up effects weakened but persisted at 6 months, and cumulative psilocybin exposure tracked larger YBOCS reductions at the end of treatment.
Source: Journal of Psychopharmacology (2026) | Moreno et al.
OCD is not simply worry turned up too high. It involves intrusive thoughts or fears, compulsive behaviors or mental rituals, and temporary relief that can reinforce the cycle.
This small randomized trial tested whether repeated psilocybin sessions could reduce measured OCD severity when standard treatments are often incomplete.
OCD Needed More Than a Single Psychedelic Session
Psilocybin has attracted attention across depression, addiction, end-of-life distress, and anxiety. OCD is a harder test case because its symptoms are repetitive, sticky, and often partially resistant to serotonin reuptake inhibitors and exposure-based therapy.
This trial did not test a casual psychedelic experience. It tested repeated dosing in a clinical research setting, with OCD severity measured by the Yale-Brown Obsessive Compulsive Scale, or YBOCS.
The trial tested more than a brief mood change. It asked whether multiple supervised sessions could reduce YBOCS scores, meaning fewer or less severe obsessions and compulsions, while remaining tolerable in a monitored research setting.
Fifteen Participants Entered a Two-Phase Dose Design
The study randomized 15 participants into three double-blind Phase 1 conditions, with five people per group. One group received high-dose psilocybin at 300 µg/kg, one received low-dose psilocybin at 100 µg/kg, and one received lorazepam as an active placebo.
Phase 1 included four weekly sessions. Then the design shifted into a single-blind Phase 2, where participants received four additional high-dose psilocybin sessions.
That structure makes the trial more informative than a single-dose case series, but it also creates interpretation limits. By the end, participants had different cumulative dose histories, and the first randomized comparison was tiny.
- High-dose arm: participants received 300 µg/kg psilocybin during the double-blind phase.
- Low-dose arm: participants received 100 µg/kg psilocybin during the double-blind phase.
- Active placebo arm: participants received lorazepam, which can produce noticeable effects without being psychedelic.
- Open dose direction: the second phase moved participants into repeated high-dose sessions, making cumulative exposure part of the result.
The Eight-Week Result Was Large for Such a Small Trial
By the end of 8 weeks, after all participants had received at least four high-dose psilocybin sessions, 73.3% met responder criteria. In this paper, response meant at least a 35% reduction in YBOCS scores.
The remission rate was also striking: 40% at the end of treatment. In a disorder where many patients get partial relief from existing options, that is the result which makes this paper newsworthy.
The randomized phase pointed in the same direction. Psilocybin, but not lorazepam placebo, significantly reduced YBOCS scores.
The active placebo matters because it gives the trial some protection against the simplest expectation-only interpretation, even though psychedelic trials remain difficult to blind fully.
YBOCS is useful here because it measures obsession and compulsion severity rather than general distress alone. A change on that scale is closer to the core disorder than a broad mood improvement.
The remission result should still be read against the denominator. Six people in remission is clinically striking, but six people is also too few to estimate how often remission would occur in a larger and more diverse OCD population.
Safety Looked Clean, But the Sample Was Tiny
The safety readout was reassuring inside the limits of the study. The authors report no serious adverse events, no psychotic symptoms, and no significant changes in suicide-severity scores.
That does not show repeated psilocybin is broadly safe for OCD outside controlled settings. The participants were treated in a clinical research environment, and the paper’s safety conclusion belongs to that context.
The sample size is the unavoidable brake on interpretation. Five people per Phase 1 condition is not enough to settle efficacy, dosing, durability, or rare adverse events.
It is enough to justify larger trials with tighter protocols.
- Safety setting: sessions occurred inside a monitored research protocol, not ordinary clinical care.
- Rare-event limit: a 15-person sample cannot estimate uncommon psychiatric or medical adverse events.
- Durability limit: follow-up suggested persistence, but the trial was too small to define relapse timing.
Safety also depends heavily on screening, preparation, monitoring, and post-session support. A supervised research protocol is not comparable to unsupervised use, especially in a disorder where anxiety, intrusive thoughts, and compulsive control can intensify under stress.
The Six-Month Signal Did Not Vanish
Researchers followed participants prospectively for 6 months. The benefits weakened after the treatment period, but they remained substantial in the study report.
That durability pattern is important because OCD symptoms often return when treatment pressure fades. A diminishing but persistent result suggests the intervention does not necessarily simply produce a short-lived post-session glow.
An exploratory cumulative-dose analysis adds another clue. Greater cumulative psilocybin dosing correlated with larger YBOCS reductions at the end of treatment, which fits the repeated-dose design but still needs prospective confirmation.
That dose pattern defines a practical problem for the next trial. Researchers need to know whether improvement depends on repeated drug exposure, repeated therapeutic contact, psychological integration after sessions, or some combination of all three.
The Next Trial Has to Separate Dose, Expectancy, and Durability
The next step is a larger randomized trial that can separate high dose from low dose, drug effect from expectancy, and acute response from sustained remission.
OCD also needs careful patient-selection work. A person with intrusive contamination fears, a person with taboo intrusive thoughts, and a person with checking rituals does not necessarily respond through the same psychological route.
For now, the study supports a narrow research claim. Repeated supervised psilocybin produced measurable YBOCS reduction in a tiny OCD sample, but it does not make psilocybin a treatment standard.
The strongest follow-up would predefine responder and remission thresholds, include a larger active-placebo control, and measure whether benefits persist after the structured session schedule ends.
It should also include enough participants to examine OCD subtype, medication background, comorbid depression, and prior exposure therapy. Those factors could change both the acute psychedelic experience and the durability of symptom relief.
Mechanistically, the next trial should measure more than YBOCS. Rumination, intolerance of uncertainty, compulsive urges, avoidance, insight, and functional impairment could reveal which parts of OCD respond first.
The cautious conclusion is still meaningful. Repeated supervised psilocybin produced measurable OCD improvement in a disorder where many people remain symptomatic despite existing treatments.
Replication will decide whether that improvement is durable enough, specific enough, and safe enough to change the OCD treatment pipeline.
Until then, the result belongs in research planning, not routine care.
Citation: DOI: 10.1177/02698811261424214. Moreno Moreno et al. A randomized clinical trial of repeated doses of psilocybin for the treatment of obsessive-compulsive disorder. Journal of Psychopharmacology . 2026. Journal of Psychopharmacology. 2026.
Study Design: Two-phase clinical trial: randomized double-blind Phase 1 with high-dose psilocybin, low-dose psilocybin, or lorazepam active placebo, followed by single-blind high-dose Phase 2.
Sample Size: 15 adults with OCD, with 5 participants per Phase 1 condition.
Key Statistic: At 8 weeks, 73.3% were responders and 40% were in remission after participants had received at least four high-dose psilocybin sessions.
Caveat: The sample was very small, and the trial cannot establish routine clinical safety, durability, or the best psilocybin dose schedule for OCD.