TL;DR: A 2026 mixed-methods study in BMC Psychiatry found that adults in psychiatric treatment valued group-based physical activity less as generic exercise and more as structured, socially supported care, with 97% of questionnaire participants saying they felt supported by activity leaders.
Key Findings
- Real-world psychiatric care: The program was embedded in an Oslo outpatient clinic for people receiving treatment for severe mental illness.
- Mixed-methods sample: Researchers combined 8 in-depth interviews with questionnaire data from 33 adults.
- Social support mattered: 97% of questionnaire participants agreed they felt supported by the activity leaders.
- Group activity fit the need: 91% wanted to stay active with other people after treatment, making social continuity a central implementation issue.
- Main caveat: The study describes participant experiences in 1 care setting; it does not test whether the program reduces symptoms compared with usual care.
Source: Hansson et al. 2026, BMC Psychiatry.
Exercise Worked as Structure, Not Just Movement
Physical activity is often discussed in mental health care as a way to improve symptoms or reduce cardiometabolic risk.
This study makes a narrower and more practical point: for people with severe mental illness, the setting around exercise may be as important as the exercise itself.
Researchers studied the Mind in Motion program at Diakonhjemmet Hospital in Oslo, Norway. The outpatient psychiatric clinic offered group-based activities such as hiking, swimming, and strength training, with patients attending 1 to 4 sessions per week.
The participants were not a general wellness sample. They were adults receiving treatment for schizophrenia spectrum disorders, bipolar disorder, psychosis, schizoaffective disorder, or other severe psychiatric conditions.
The study used a qualitative-driven mixed-methods design. That means the interviews carried much of the explanation, while questionnaire data helped show whether the same patterns appeared across a broader group.
- Interview group: 8 active program participants completed semi-structured interviews.
- Questionnaire group: 33 participants contributed survey data, including the interview participants.
- Care setting: The activity program was part of routine psychiatric treatment, not a separate fitness trial.
- Program dose: Participants reported an average of 2.0 activity days per week, with a range from 1 to 4.
The Main Benefits Were Well-Being, Belonging, and Routine
The researchers organized the findings around 3 areas: perceived health benefits, barriers, and transition after treatment. Within those areas, they constructed 8 themes from the interview data and integrated the questionnaire results.
The first cluster was broad health benefit. Participants described activity as a way to feel better, regain momentum, spend time outdoors, and experience a sense of accomplishment after showing up.
The social piece was not secondary. Several participants described the group as a source of belonging, and being expected by other people helped turn intention into attendance.
The third benefit was routine. For people whose days can be shaped by symptoms, treatment schedules, unemployment, fatigue, or isolation, a set activity time gave the week a more predictable structure.
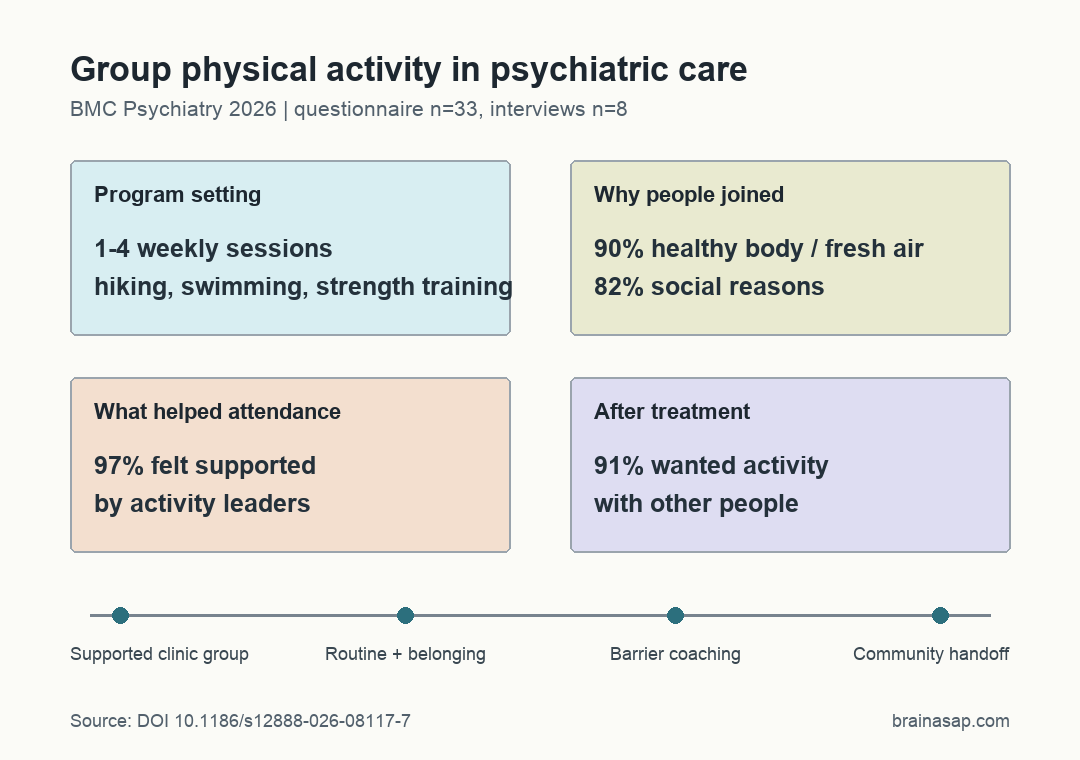
The survey results lined up with that interpretation. 90% of participants said they joined to have a healthy body and get fresh air. 82% also reported social reasons for participation.
Participants rated the perceived positive effect of the program at 7.9 out of 10 for physical health and 7.7 out of 10 for mental health. Those numbers are not symptom-outcome scores, but they show that participants experienced the program as meaningful across both domains.
Barriers Were Clinical, Practical, and Motivational
The study is useful because it does not pretend that telling patients to exercise is enough. Participants described barriers that are common in severe mental illness and psychiatric medication use.
- Medication side effects: Fatigue, sluggishness, and weight gain could lower energy and motivation.
- Sleep and symptoms: Poor sleep, fluctuating mental state, and low motivation could make attendance harder.
- Practical conditions: Seasonal weather, logistics, and discomfort around being in an illness-defined group could also matter.
Those barriers point to a design lesson. A physical activity program in psychiatric care needs enough flexibility to meet people on low-energy days while still offering predictable structure.
The activity leaders were the clearest facilitator. They adapted activities, followed up with patients, reduced practical barriers, and helped create a safe group climate.
That role was visible in the questionnaire data. 97% of participants agreed that they felt supported by activity leaders, and participants reported missing an average of only 0.9 sessions per month.
The Weak Point Was What Happens After Treatment
The study’s most actionable finding comes after the hospital program ends. Participants often wanted to remain active, but moving from a supported treatment setting to community options was not straightforward.
Some participants knew about alternatives, and 63.6% of questionnaire participants reported awareness of community options. But the interviews suggested that a list of activities was not enough when people still needed social support, encouragement, and a setting that felt psychologically safe.
The strongest number here is the social-continuity result: 91% wanted to be active with others in some form after treatment.
For this group, continuity was not just access to a gym or trail. It was access to a realistic social bridge.
- For clinics: Physical activity programs may need planned handoffs into community groups, not just discharge advice.
- For researchers: The next step is testing which supports help people stay active after structured psychiatric care.
- For interpretation: The program’s value appears to come from movement plus leadership, group belonging, and routine.
This is not evidence that group physical activity alone treats schizophrenia, bipolar disorder, or psychosis. It is evidence that patients in 1 real-world psychiatric service experienced tailored group activity as a useful part of care, while also identifying the support needed to keep going.
Citation: DOI: 10.1186/s12888-026-08117-7. Hansson Mind in motion: patients’ experiences with group-based physical activity in psychiatric treatment- a mixed-methods study. BMC Psychiatry. 2026.
Study Design: Qualitative-driven mixed-methods study in a real-world outpatient psychiatric physical activity program.
Sample Size: 33 questionnaire participants, including 8 adults who completed in-depth interviews.
Key Statistic: 97% of questionnaire participants agreed they felt supported by activity leaders; 91% wanted to stay active with others after treatment.
Caveat: The study reports experiences and perceived benefits in 1 Norwegian treatment setting, not a controlled test of symptom or health outcomes.