TL;DR: A 2026 medRxiv preprint found that soluble CD27 (sCD27), a T-cell activation marker, was elevated in a subgroup of patients with severe psychiatric disorders and was more common when autoimmune disease or abnormal cerebrospinal fluid (CSF) inflammation markers were present.
Key Findings
- The immunopsychiatry cohort included 115 patients: Researchers compared severe psychiatric-disorder cases enriched for suspected immune involvement with 37 multiple sclerosis patients and 154 surgical controls.
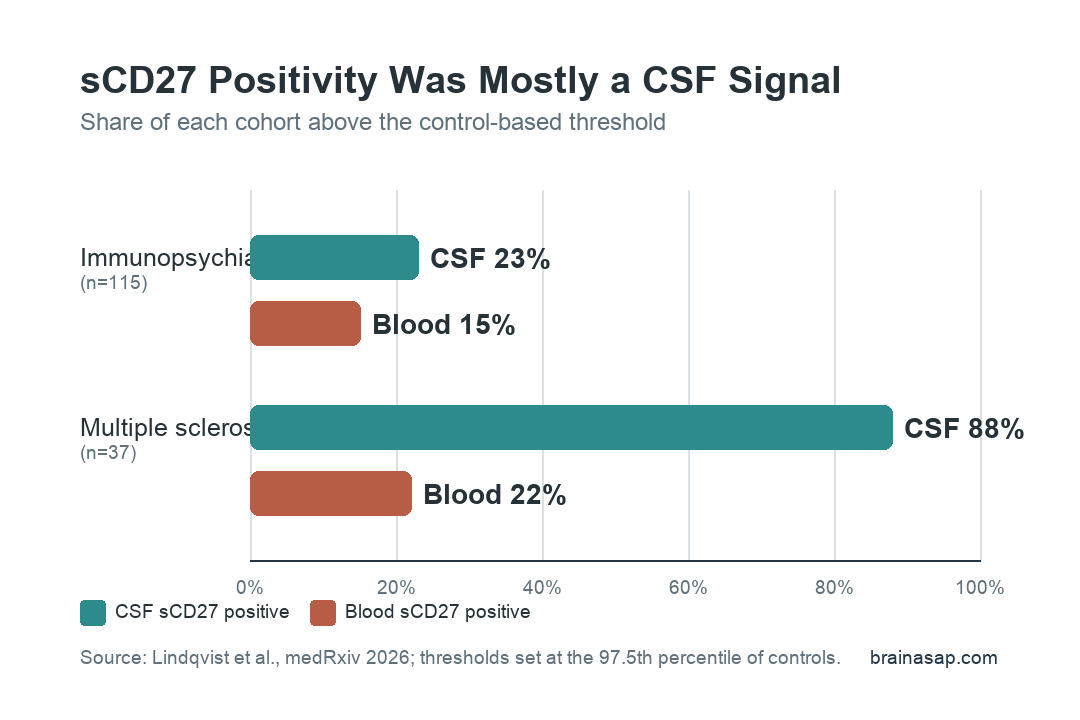
- Cerebrospinal fluid (CSF) sCD27 positivity appeared in 23% of psychiatric cases: The same fluid marker was positive in 88% of the multiple sclerosis comparison group, supporting it as a central neuroinflammation signal.
- Autoimmune disease was more common when sCD27 was positive: Combined CSF and/or blood sCD27 positivity was associated with comorbid autoimmune disease (chi-square = 8.56, p = 0.003).
- CSF sCD27 tracked other inflammation markers: Positive cases were more likely to show pleocytosis, elevated total tau, elevated neurofilament light, or another abnormal cerebrospinal-fluid finding.
- The marker is not a psychiatric screening test: The cohort was clinically enriched for immune suspicion, and the preprint was not peer reviewed, so the finding points to a subgroup for specialist evaluation rather than routine testing.
Source: Lindqvist et al. medRxiv. 2026.
Autoimmune disease can sometimes enter psychiatric care indirectly: mood symptoms, psychosis, obsessive-compulsive symptoms, cognitive change, or catatonia may appear before the immune diagnosis is obvious.
Researchers tested whether soluble CD27 (sCD27), a marker released during T-cell activation, could help separate immune-linked cases from the broader severe-psychiatry group.
The study focused on a clinically selected immunopsychiatry cohort. These were not unselected clinic patients.
They had severe psychiatric symptoms plus clinical signs that raised concern for possible immune involvement, which makes the result useful but limits how broadly it can be applied.
Soluble CD27 Measured T-Cell Activation in CSF and Blood
sCD27 is the soluble form of CD27, a receptor involved in T-cell and B-cell immune signaling. In neurology, cerebrospinal-fluid sCD27 has been studied as a marker of intrathecal T-cell-mediated inflammation, especially in multiple sclerosis.
Researchers measured sCD27 in two compartments:
- Cerebrospinal fluid (CSF): the fluid surrounding the brain and spinal cord, used here as the central nervous system compartment.
- Blood: the peripheral compartment, used to catch systemic immune activation that might not appear in CSF.
- Age-stratified cutoffs: positivity was defined above the 97.5th percentile of surgical controls, separately for younger and older groups.
The compartment split was clinically important. Several high-CSF cases were blood-negative, including patients later found to have multiple sclerosis. A blood-only approach would have missed those central immune findings.
CSF sCD27 Was Positive in 23% of Psychiatric Cases
In the 115-patient immunopsychiatry cohort, 23% were positive for CSF sCD27 and 15% were positive for blood sCD27. In the multiple sclerosis comparison group, 88% were CSF-positive and 22% were blood-positive.
This comparison helps anchor the psychiatric finding. The marker behaved as expected in a neurological inflammatory disease.
A subset of severe psychiatric cases also had CSF values above the control reference range, though not as uniformly as the multiple sclerosis group.
The psychiatric diagnoses themselves did not sort cleanly by sCD27 status. Positive cases appeared across different psychiatric presentations rather than clustering around one diagnosis such as psychosis, obsessive-compulsive symptoms, mood symptoms, or catatonia.
Autoimmune Disease Was Linked to Positive sCD27
The clinically important pattern was not a psychiatric label. It was autoimmune comorbidity. In the immunopsychiatry cohort, 34 patients already had autoimmune disease at sampling, and additional cases were diagnosed later during follow-up.
Combined CSF and/or blood sCD27 positivity was associated with comorbid autoimmune disease. The association was stronger for the combined marker than for blood alone:
- Combined CSF and/or blood sCD27: associated with autoimmune disease (chi-square = 8.56, p = 0.003).
- CSF sCD27 alone: also associated with autoimmune disease (chi-square = 4.85, p = 0.028).
- Blood sCD27 alone: did not identify autoimmune disease as well in this cohort (chi-square = 1.35, p = 0.245).
Ordinal logistic regression also linked CSF sCD27 positivity to autoimmune disease activity, with an odds ratio of 5.14. That does not prove the psychiatric symptoms were autoimmune in origin.
It does strengthen the case that sCD27 was capturing clinically meaningful immune activity rather than random lab variation.
CSF Abnormalities Supported a Neuroinflammation Signal
Positive sCD27 cases were also more likely to have other abnormal CSF findings. Researchers reported associations with pleocytosis, meaning increased white blood cells in CSF; elevated total tau, a marker of neuronal injury or stress; and elevated neurofilament light, a marker of axonal injury.
Several details make the finding worth taking seriously:
- All pleocytosis cases were CSF-sCD27 positive: Blood sCD27 was negative in those same four cases, pointing to central rather than peripheral activity.
- Any abnormal CSF marker was more common in sCD27-positive patients: The combined CSF-abnormality comparison reached p = 0.003.
- Fifteen sCD27-positive patients had no known autoimmune diagnosis: Some also had other abnormal CSF markers, raising the possibility of immune activity that did not yet fit a standard disease category.
That last point is the most cautious interpretation of the study. The marker may help flag patients who may need autoimmune or neuroinflammatory evaluation, especially when psychiatric symptoms appear with acute onset, neurological symptoms, seizures, abnormal CSF, or other red flags.
The Marker Still Needs Broader Validation
This was an enriched clinical cohort, not a population screen. Psychiatric patients were selected because immune involvement was already suspected, so the 23% CSF-positive rate should not be projected onto all psychiatric patients.
Other limits are practical and clinical:
- CSF testing is invasive: Lumbar puncture is not a routine psychiatric test and should be reserved for specialist indications.
- The preprint is not peer reviewed: Results may change after review or replication.
- Autoimmune causality was not proven: sCD27 positivity can mark immune activity without proving it caused the psychiatric syndrome.
- The cohort was heterogeneous: Different autoimmune diseases, psychiatric presentations, and illness courses were analyzed together.
The useful clinical framing is narrower: in severe psychiatric cases where autoimmune or neurological red flags already exist, combined CSF and blood sCD27 may become one more piece of evidence for immune-system involvement.
Citation: DOI: 10.64898/2026.04.16.26351038. Lindqvist et al. Soluble CD27 as an indicator of autoimmune disease in severe psychiatric disorders. medRxiv. 2026.
Study Design: Cross-sectional biomarker comparison of a clinically enriched immunopsychiatry cohort, multiple sclerosis positive-control cohort, and surgical controls.
Sample Size: 115 immunopsychiatry patients, 37 multiple sclerosis patients, and 154 surgical controls.
Key Statistic: Combined CSF and/or blood sCD27 positivity was associated with comorbid autoimmune disease in the psychiatric cohort (chi-square = 8.56, p = 0.003).
Caveat: The preprint was not peer reviewed, and the psychiatric cohort was enriched for suspected immune involvement rather than sampled from general psychiatric practice.