TL;DR: A 2026 qualitative study in BJPsych Open found that mental-health stigma in Ethiopia’s Somali Regional State shaped how people recognized illness, delayed biomedical care-seeking, and reinforced neglect of mental-health services.
Key Findings
- Sixteen interviews anchored the study: Researchers interviewed health workers, service users, carers, and community-facing professionals in Jigjiga and Kabridahar.
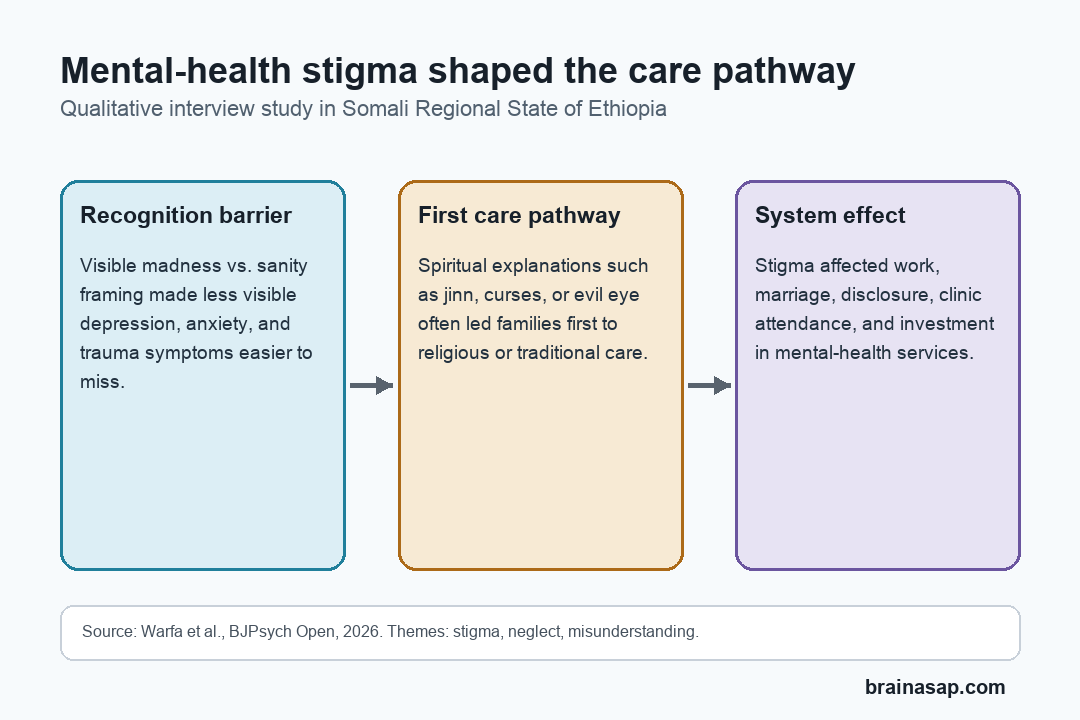
- Mental illness was often framed as binary: Participants described a common view that a person is either “mad” or sane, leaving depression, anxiety, and other less visible conditions poorly recognized.
- Spiritual explanations shaped care-seeking: Many participants said families often sought religious or traditional treatment first, especially when illness was attributed to jinn, witchcraft, curses, or evil eye.
- Stigma affected work, marriage, and trust: People with mental-health conditions were described as being excluded from ordinary social roles and sometimes hidden by families.
- Service neglect was part of the same pattern: Participants argued that stigma toward people with mental illness also lowered investment in mental-health facilities and care pathways.
Source: Warfa et al. 2026 BJPsych Open study.
Mental-health care is not only limited by the number of clinics or clinicians. In some settings, the first barrier is whether distress is recognized as a treatable health condition at all.
This study focused on the Somali Regional State of Ethiopia, a large region with more than 6 million people and a mental-health system still developing after decades of conflict, poverty, displacement, and underinvestment.
In 2022, the region had only one psychiatrist and about 20 psychiatric nurses, according to the paper’s background. The interviews suggest that workforce numbers are only one part of the problem.
Sixteen Interviews Mapped Stigma and Care-Seeking
The researchers conducted 16 semi-structured interviews between April and July 2024 in Jigjiga, the regional capital, and Kabridahar, the region’s third-largest city.
The sample was small but intentionally varied. It included service users, carers, nurses, psychiatric nurses, a psychiatrist, a general practitioner, and a non-specialist doctor.
A pharmacist, a mental-health volunteer, and other front-line or community-facing participants also contributed.
The interviews were translated, transcribed, coded in NVivo 14, and analyzed with thematic analysis. Three broad themes organized the results:
- Mental-health stigma: How people with mental-health conditions were labeled, excluded, hidden, or mistreated.
- Societal neglect: How low social priority for mental health affected services and investment.
- Misunderstanding of illness: How mental distress was interpreted through visible behavior, spiritual explanations, or ideas of incurability.
The study is best read as a qualitative map of barriers, not as a prevalence estimate. It does not tell readers how common each belief is across the whole region, but it shows how the barriers can fit together.
Binary Views Made Less Visible Conditions Easier to Miss
A central finding was the reported tendency to divide mental health into a simple binary: a person was either visibly “mad” or not mentally ill.
In that model, severe psychosis-like presentations were more likely to be recognized, while depression, anxiety, post-traumatic stress, or obsessive-compulsive symptoms could be treated as something else.
The distinction affects timing. If mental illness is acknowledged only after behavior becomes highly visible, families may wait until a condition is advanced before seeking biomedical care.
Several professionals in the study said community understanding often focused on overt public behavior, homelessness, danger, or the need to restrain someone. A less visible condition could remain private, unnamed, or morally interpreted.
The researchers also described the idea that mental illness was often considered incurable. That belief can make treatment seem pointless and can keep a recovered person from regaining trust or status even after symptoms improve.
Spiritual Explanations Often Came Before Biomedical Care
Participants repeatedly described spiritual explanations for mental illness. These included jinn, witchcraft, curses, evil eye, and other religious or traditional interpretations.
Spiritual care may still be part of local life. The practical issue is the order and consequences of care-seeking.
When distress is understood mainly as spiritual, families may first seek help from religious or traditional providers and use biomedical care only after other options have failed.
The reported care pathway often moved through several steps:
- Family interpretation: Relatives or carers decide what the problem means and where help should be sought.
- Religious or traditional treatment: The first response may involve Sheikhs, Quran readings, traditional medicine, or inpatient religious care facilities known as ilaajs.
- Delayed clinic contact: Hospital or outpatient mental-health care may become the last resort rather than the first medical option.
This delay is especially important in a region where biomedical services are already sparse. A thin care system becomes even harder to use when people fear the label attached to it.
Stigma Reached Work, Marriage, and Service Investment
Stigma was not described as a single attitude. Participants connected it to violence, ridicule, exclusion, hiding illness, loss of work, reduced marriage prospects, and loss of trust in a person’s decision-making.
Some participants described families concealing illness at home to avoid public labeling. Others described people avoiding outpatient departments because being seen there could identify them as mentally ill.
The same logic extended to services. A participant’s phrase, used in the paper title, captured the point: when people with mental illness are stigmatized, the service for them can be stigmatized too.
That creates a feedback loop:
- Low recognition: Less visible mental-health problems are missed or minimized.
- Late help-seeking: Families often exhaust non-biomedical options before seeking formal care.
- Public labeling: Clinic attendance itself can become socially risky.
- Service neglect: Low priority for mental-health care reinforces weak facilities and poor access.
The study’s most useful contribution is this system-level view. Stigma affects individual patients, but it also shapes whether a health system is funded, trusted, and used.
Service-User Voices Were Harder to Capture
The researchers were explicit about a major limitation: the findings were dominated by professional participants. Recruiting service users and carers was difficult, and power differences may have limited how fully service users expressed their views.
That limitation is not just a methods note. It is part of the finding.
If stigma makes people with mental-health conditions harder to recruit and less likely to speak freely, then future service design needs more than clinic expansion.
Practical improvement would likely need several linked pieces:
- Community education: Naming depression, anxiety, trauma symptoms, and other less visible conditions as treatable health problems.
- Respectful care pathways: Making clinics feel safe enough that attendance does not become another stigma exposure.
- Service-user involvement: Including people with lived experience in designing services, not only as recipients of care.
- Cultural fit: Engaging local explanatory models without letting delayed or harmful care become the default pathway.
The finding is not that one belief explains every care delay. Poverty, medication access, distance to facilities, workforce shortages, and long-term illness burden also matter.
The study argues that stigma sits across all of those barriers. It affects how illness is named, who gets trusted, when care is sought, and whether mental-health services are treated as a public priority.
Citation: DOI: 10.1192/bjo.2026.11016. Warfa et al. Since people who have mental illness are stigmatised, their service is also stigmatised. You get a massive hospital building and there is no mental health facility: exploring perceptions of mental health, stigma of mental illness, care-seeking and service use in the Somali Regional State of Ethiopia. BJPsych Open. 2026.
Study Design: Qualitative interview study using translated transcripts and thematic analysis.
Sample Size: 16 adult participants, including health workers, service users, carers, and community-facing professionals in Jigjiga and Kabridahar.
Key Statistic: The paper’s background notes that, in 2022, one psychiatrist and about 20 psychiatric nurses covered the Somali Regional State.
Caveat: Service-user and carer perspectives were harder to recruit and elaborate, so professional viewpoints shaped much of the final analysis.