TL;DR: A 2026 preprint in medRxiv from the CORE-VNS study reported that vagus nerve stimulation (VNS), a neuromodulation therapy for drug-resistant epilepsy, produced similar 36-month seizure reductions in people with and without prior intracranial epilepsy surgery.
Key Findings
- 531 VNS implants: The analysis included 531 people with drug-resistant epilepsy who received an initial VNS implant in the prospective CORE-VNS study.
- 84 prior surgeries: Prior intracranial surgery for epilepsy (ICSE) was recorded in 84 participants, while 447 had no such history.
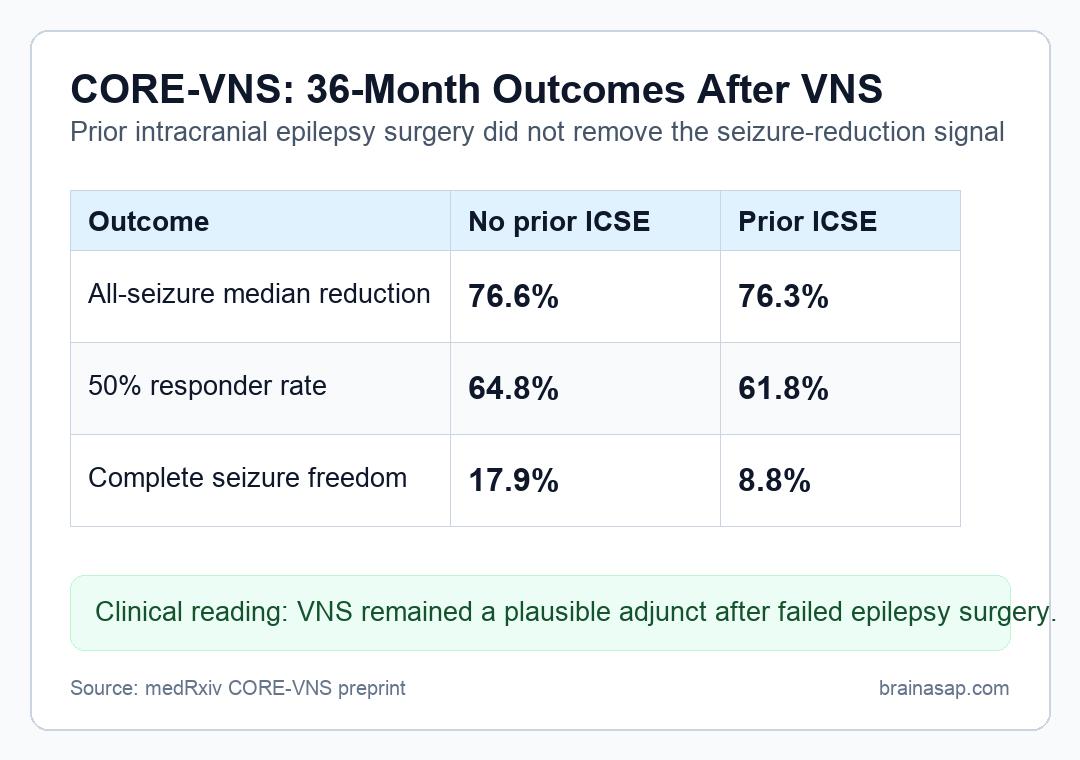
- Similar all-seizure reductions: Median all-seizure reduction at 36 months was 76.6% without prior ICSE and 76.3% with prior ICSE.
- Responder rates matched: At least 50% seizure reduction was reported in 64.8% without prior ICSE and 61.8% with prior ICSE.
- Seizure freedom differed numerically: Complete seizure freedom was reported in 17.9% without prior ICSE and 8.8% with prior ICSE.
Source: medRxiv (2026) | Nicolai et al.
Vagus nerve stimulation (VNS) sends intermittent electrical stimulation through the vagus nerve and is used when drug-resistant epilepsy continues despite antiseizure medications. In some patients, VNS is considered only after epilepsy surgery has not produced seizure freedom.
The CORE-VNS analysis compared patients who had already undergone intracranial surgery for epilepsy with those who had not. It did not treat prior surgery as a reason to exclude people from the VNS outcome comparison.
CORE-VNS Followed 531 People After VNS Implantation
CORE-VNS was a prospective, multicenter, international observational study. Participants received an initial VNS implant and were followed for seizure and non-seizure outcomes at 3, 6, 12, 24, and 36 months.
The analysis separated people by history of intracranial surgery for epilepsy (ICSE). ICSE included procedures such as resection, disconnection surgery, or intracranial neuromodulation used before VNS.
- No prior ICSE: 447 participants had no recorded history of intracranial epilepsy surgery before VNS.
- Prior ICSE: 84 participants had previous intracranial surgery and still needed additional seizure treatment.
- Main comparison: Researchers compared baseline characteristics, 36-month seizure outcomes, and safety patterns between the two groups.
This design cannot randomize people to surgery history, but it can address a practical sequencing issue. Clinicians often need to know whether VNS remains reasonable after surgical treatment has already failed to control seizures.
36-Month Seizure Reductions Were Similar With or Without Prior Surgery
The headline seizure result was close across groups. Median all-seizure reduction at 36 months was 76.6% in people without prior ICSE and 76.3% in those with prior ICSE.
Focal and generalized seizure categories showed the same broad pattern. All focal seizures fell by a median of 83.3% without prior ICSE and 71.8% with prior ICSE, while all generalized seizures fell by 77.8% and 76.2%, respectively.
- All seizures: Nearly identical median reduction, separated by only 0.3 percentage points.
- Focal seizures: Numerically higher reduction in the no-prior-surgery group, but still substantial in both groups.
- Generalized seizures: Median reductions were almost the same across prior-surgery status.
The core interpretation is that prior intracranial surgery did not erase VNS-associated seizure reduction in this cohort. People with previous surgery still showed clinically large median reductions.
50% Responder Rates Were Close Across Surgery History
The 50% responder measure asks how many participants cut seizure frequency by at least half from baseline. That threshold is common in epilepsy neuromodulation studies because complete seizure freedom is harder to achieve.
Responder rates were similar: 64.8% in participants without prior ICSE and 61.8% in those with prior ICSE. Complete seizure freedom was lower in the prior-ICSE group, at 8.8% compared with 17.9%.
- Responder interpretation: The main clinical improvement threshold looked similar across groups.
- Seizure-freedom interpretation: The prior-surgery group had a lower numerical seizure-freedom rate, which may reflect a harder-to-treat subgroup.
- Patient-level caution: A median or responder rate does not predict an individual person’s VNS response.
The distinction is clinically important. The analysis supports considering VNS after failed surgery, but it does not promise seizure freedom after VNS.
Safety Results Did Not Show a Prior-Surgery Penalty
The report also compared implant-related adverse events and serious adverse events. Rates were described as similar between participants with and without prior ICSE.
Historical labeling for VNS noted that safety and efficacy had not been established in people with prior brain surgery. The CORE-VNS data address that uncertainty with a larger contemporary cohort.
- Mechanism context: VNS sends sensory vagus-nerve input to brainstem nuclei, then broader neuromodulatory systems, rather than stimulating a prior surgical site directly.
- Label context: Earlier pivotal VNS studies did not include enough prior-surgery patients to evaluate them well.
- Clinical context: Persistent seizures after surgery often leave patients needing additional options.
Safety similarity does not remove the need for individualized surgical and device-risk review. It does weaken the idea that prior intracranial epilepsy surgery alone should rule out VNS consideration.
The Preprint Supports VNS Consideration After Failed Epilepsy Surgery
The cleanest clinical conclusion is about contraindication logic. In this CORE-VNS analysis, prior ICSE did not meaningfully change 36-month median seizure reduction or responder rates after VNS implantation.
The main limits are also clear. This was an observational analysis, not a randomized comparison of treatment sequences, and the prior-surgery group was smaller than the no-prior-surgery group.
- Design limit: People with prior surgery may differ from people without prior surgery in epilepsy type, severity, prior treatment course, and surgical candidacy.
- Evidence status: The source is a medRxiv preprint and has not completed peer review.
- Actionable reading: Prior ICSE should be part of counseling, but not treated as an automatic reason to avoid VNS.
For refractory epilepsy care, the clinical use is sequencing. When seizures continue after surgery, VNS remains a plausible adjunctive option to discuss in a comprehensive epilepsy center.
Citation: DOI: 10.64898/2026.04.17.26351099. Nicolai et al. Vagus Nerve Stimulation in Failed Epilepsy Surgery: 36 Month Outcomes From the CORE-VNS Study. medRxiv. 2026.
Study Design: Prospective multicenter observational CORE-VNS analysis comparing VNS outcomes by prior intracranial epilepsy-surgery history.
Sample Size: 531 people with drug-resistant epilepsy, including 84 with prior intracranial surgery for epilepsy.
Key Statistic: Median all-seizure reduction at 36 months was 76.6% without prior ICSE and 76.3% with prior ICSE.
Caveat: The study was observational and the source was a preprint, so treatment sequencing should still be individualized.





